Downloaded 1,011 times
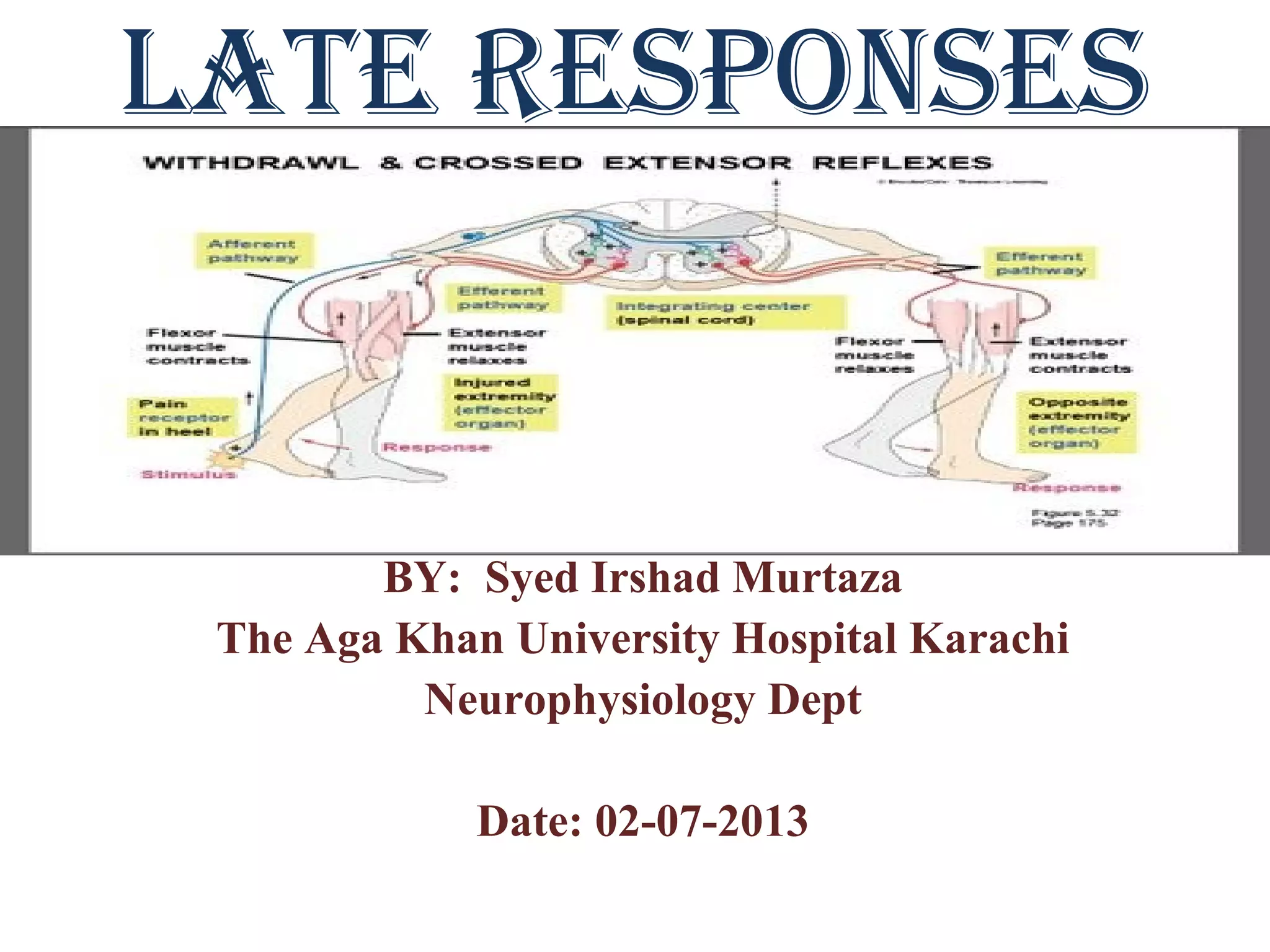
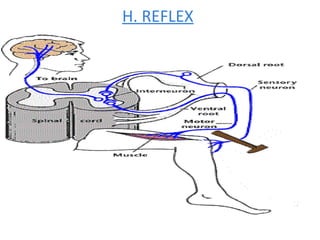
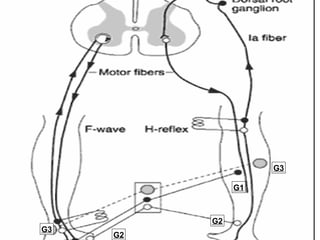
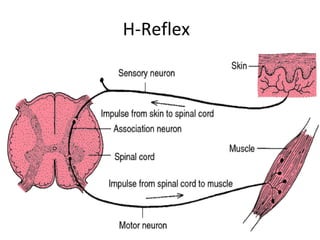
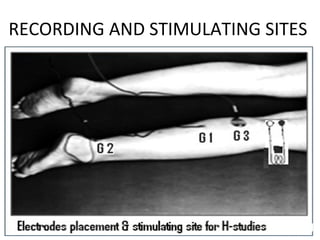
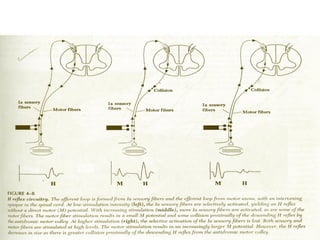
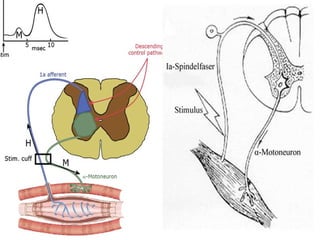
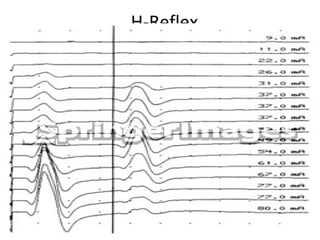
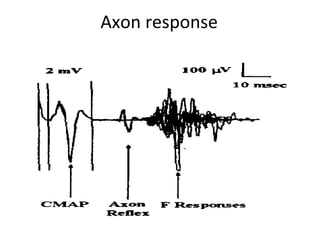
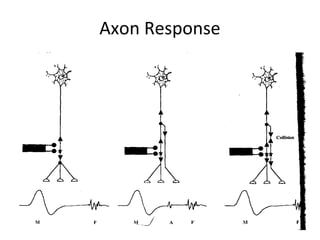
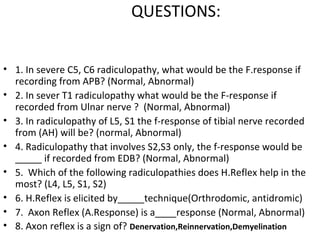

This document provides information about late responses in nerve conduction studies, including F-waves, H-reflexes, and axon reflexes. It discusses the mechanisms, characteristics, and clinical applications of each response. The F-wave results from antidromic stimulation of motor neurons and evaluates more proximal nerve segments. The H-reflex is a monosynaptic stretch reflex that is reliably measured in the lower limbs. Axon reflexes occur due to terminal nerve branching and suggest reinnervation. Late responses provide valuable information about radiculopathies and plexopathies that cannot be observed with distal nerve studies alone.



























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













