04/29/2025 3
Introduction
• Nerveis basic unit of peripheral nervous system.
• With in a nerve each axon is surrounded by layer of
connective tissue called endoneurium
• Axons are bundled together in to groups called fascicles.
• Each fascicle is surrounded by connective tissue called
perineurium.
4.
04/29/2025 4
• Theentire nerve is covered by a connective tissue layer called
epineurium.
• Perineurium is a layer of fatty cells.
• The endoneurium contains low protein liquid called
endoneurial fluid.
5.
04/29/2025 5
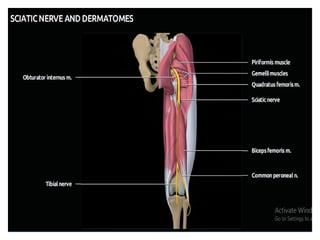
Nerves oflower extremity
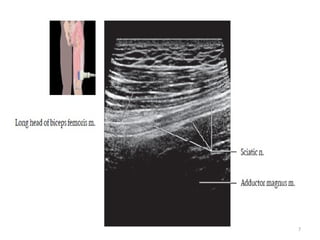
Sciatic nerve
• Arises from L4, L5, S1, S2, S3, branches of sacral plexus.
• It’s the longest and widest nerve in the body.
• Two nerves (common peroneal and tibial) bound together.
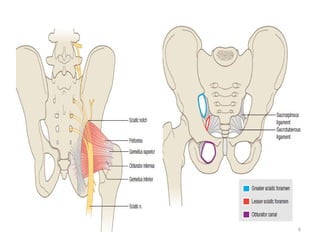
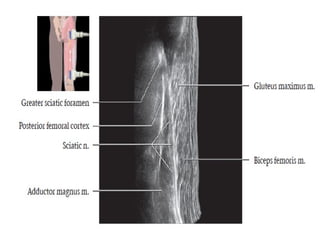
• Exits pelvis through the greater sciatic foramen inferior to
piriformis muscle.
04/29/2025 8
• Crossesover superior gemellus, obturator internus, inferior
gemellus muscles.
• It is deep to long head of biceps femoris muscle.
• Branches arising in thigh:
- Articular to hip,
- Nerves to hamstring muscles
04/29/2025 13
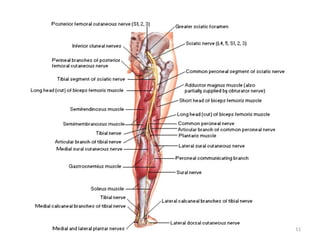
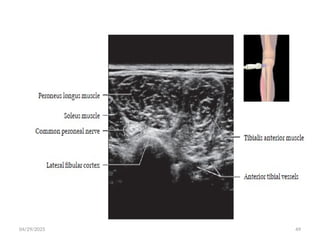
CommonPeroneal Nerve
• Also known as common fibular nerve and forms lateral part of
sciatic nerve.
• Smaller of 2 terminal divisions of sciatic nerve.
• Arises from dorsal divisions of sacral plexus (L4-S2)
• Separates from tibial nerve at superior angle of popliteal fossa.
04/29/2025 16
• Leavespopliteal fossa by crossing plantaris and lateral head of
gastrocnemius.
• Oblique lateral course with biceps femoris muscle.
• Innervates short head of biceps femoris muscle.
• Ends between lateral side of neck of fibula and peroneus
longus.
17.
04/29/2025 17
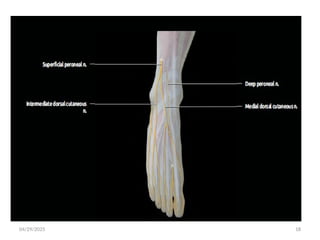
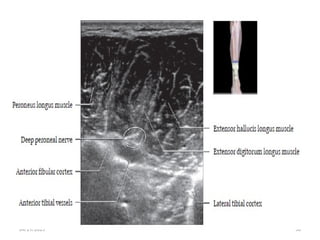
• Dividesinto its two terminal branches in the peroneus longus
muscle.
1.superficial peroneal nerve
2.deep peroneal nerve
Other branches are:
-Peroneal communicating nerve
-Lateral sural cutaneous nerve
-Superior and inferior genicular nerves
-Recurrent genicular nerves
-Muscular branches
04/29/2025 20
Motorsupply:
• short head of biceps femoris.
• muscles of the extensor compartment of the leg by deep peroneal nerve.
• Muscles of the lateral compartment of the leg by superficial peroneal nerve
Sensory supply: cutaneous innervation of posterolateral leg.
Fibular neck fracture may result in foot drop.
21.
04/29/2025 21
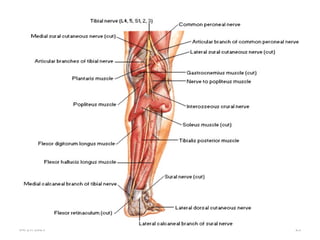
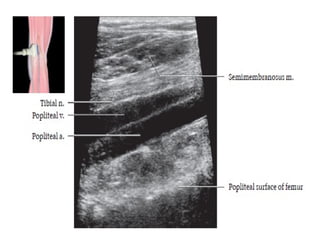
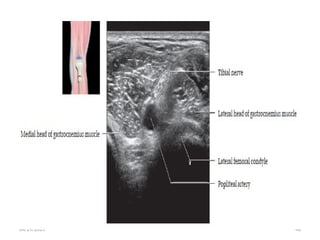
Tibial Nerve
•Largest division of sciatic nerve.
• Arises from ventral surface of sacral plexus(L4-S3) and runs
medially.
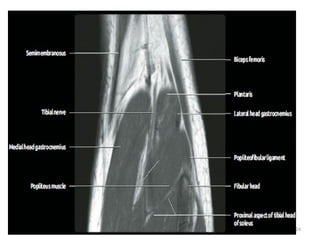
• Courses through the popliteal fossa passing deep to
gastrocnemius muscle.
22.
04/29/2025 22
• Itpasses inferiorly between the heads of gastrocnemius and
deep to soleus muscle.
• Continues inferiorly in the midline deep to soleus and
superficial to the tibialis posterior muscle.
• At the ankle passes under flexor retinaculum in the tarsal
tunnel.
04/29/2025 26
• Atthe level of medial malleolus it divides into three terminal
branches.
1.medial plantar nerve
2.lateral plantar nerve
3.medial calcaneal nerve
27.
04/29/2025 27
• Motorsupply:
- posterior thigh muscles except short head of biceps femoris
muscle.
- Posterior compartment of the leg
- Muscles of the sole of the foot
Sensory supply:
-Articular branches to knee, ankle and foot joints
-Cutaneous branches to posterior calf and sole of the foot
28.
04/29/2025 28
Sural Nerve
•Sensory nerve of the lower limb.
• Its formed by the union of sural branch of tibial nerve and
communicating sural branch of common fibular nerve.
• Travels within subcutaneous tissue adjacent to small saphenous vein.
• It descends behind the lateral malleolus and becomes lateral dorsal
cutaneous nerve.
04/29/2025 31
Itcontains nerve roots of S1 and S2 and provides sensation to:
Lower lateral calf
Lateral ankle
Lateral foot and some of the 5th
digit
Sural communicating branch of common peroneal nerve is
absent in 20% of the population.
Injury to this nerve is well tolerated and its often used for nerve
grafting or biopsy.
32.
04/29/2025 32
FemoralNerve
• Arises from posterior divisions of L2-L4 roots of the lumbar plexus.
• Largest branch of lumbar plexus.
• It emerges from the lateral boarder of the psoas muscle and medial boarder of
iliacus muscle.
• It sends motor branch to iliacus before passing under the inguinal ligament to
enter femoral triangle.
• Exits pelvis beneath inguinal ligament, lateral to femoral vessels, enters femoral
triangle.
33.
04/29/2025 33
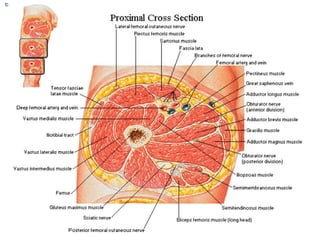
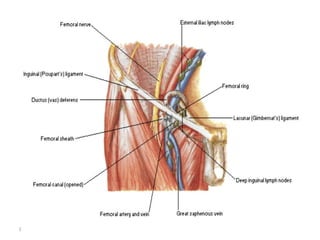
Femoral triangle
•Anatomical space in the anterior upper thigh that contains
several structures.
The boundaries are:
• Laterally medial border of Sartorius
• Medially medial border of adductor longus
• Superiorly inguinal ligament
• Floor ilopsoas laterally and pectineus medially
• Roof skin and subcutaneous tissue
04/29/2025 37
Motor supply
-Anteriorcompartment of the thigh
Sensory supply
-Hip
-Anterior and medial thigh
-Knee and medial leg as saphenous nerve
The femoral nerve is responsible for patellar tendon reflex (tests L3-
L4spinal component).
38.
04/29/2025 38
Proximal branches
Branchesto iliacus before crossing inguinal ligament
Nerve to pectineus after crossing inguinal ligament
Branches of superficial division
Nerve to Sartorius
Anterior femoral cutaneous nerve
Sympathetic vasomotor supply to blood vessels
Deep division
Nerve to anterior compartment of thigh muscles
Saphenous nerve which passes behind Sartorius
39.
04/29/2025 39
• SaphenousNerve
• It’s the continuation of deep division of the femoral nerve in the
femoral triangle.
•
• Longest branch of femoral nerve, arising 2 cm below inguinal
ligament and descending via adductor canal.
• Passes posterior to Sartorius, descends posteromedial to knee where
it pierces deep fascia.
• In leg accompanies great saphenous vein.
40.
04/29/2025 40
Imaging
• Onplain radiographs nerves are characterized
by non specific soft tissue density.
• On CT scan nerves are characterized by soft
tissue density structures.
41.
04/29/2025 41
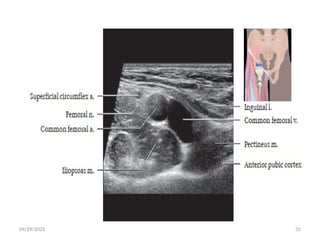
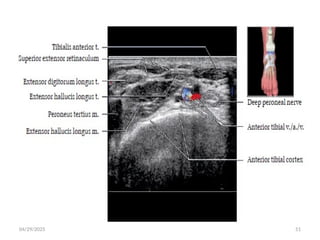
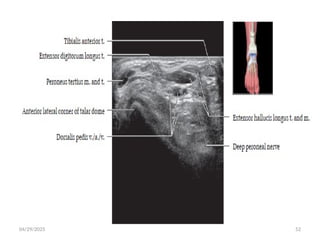
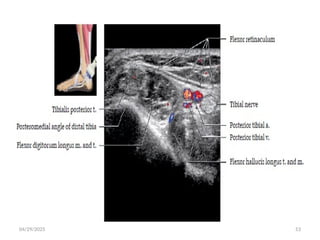
Ultrasound
Use high-frequency transducers to assess nerves.
Short axis: A typical “honeycomb” appearance with hypoechoic
fascicles and surrounding echogenic perineurium
Long axis: Parallel hypoechoic tracts of uniform caliber.
Distortion of this uniform appearance suggests pathology
42.
04/29/2025 42
• Tracemedium-sized nerves by following their course as they
branch from their parent.
• Small (1-2 mm) nerves are difficult to identify and location
may only be inferred by adjacent vessels.
04/29/2025 54
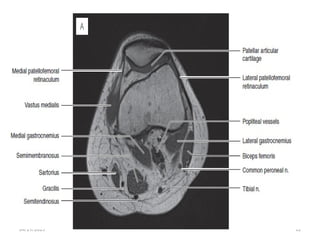
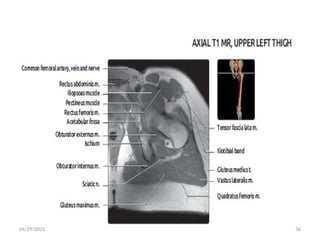
MRI
T1or PD help distinguish fluid in vessels from
nerves.
Correlate with fluid-sensitive sequences.
Fat fascicles are especially prominent in
sciatic nerve.
55.
04/29/2025 55
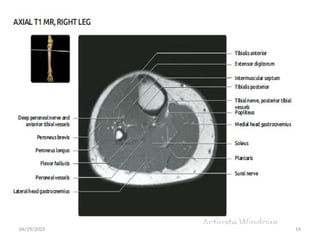
• Theabundant fat around the fascicles and the nerve itself
makes these structures clearly visible on T1-weighted images.
• Normal fascicular shape was defined as clustered similar-sized
rounded structures on T1 MR images.
56.
04/29/2025 56
• Thenormal nerve shows a fascicular appearance.
• It has signal intensity from isointense to minimally
hyperintense with respect of the adjacent muscle.
• The perineural fat tissue has a homogeneous signal and a
separation plane with the adjacent structures.
04/29/2025 61
Accessory piriformismuscle: rare variant
• Accessory muscle slips covering sacral foramina/sacral
nerves
• Two distinct muscle bellies fusing to form a common
tendon
• Accessory slips arising from the sacro tuberous ligament
62.
04/29/2025 62
• Threemuscle bellies
• Accessory slip arising from the main muscle
belly with separate tendinous insertion in to
greater trochanter.
• Piriformis syndrome
63.
04/29/2025 63
Accessory femoralnerve: fibers arise separately in
lumbar plexus passes anterior to femoral nerve may
terminate as saphenous nerve.
• Saphenous nerve may terminate at knee with distribution
replaced by branch of tibial nerve.
• Femoral nerve splits into two or three separate slips with in
psoas muscle but united to descend as single bundle.
64.
04/29/2025 64
References
• AppliedRadiological Anatomy Second Edition
• FRANK H.. NETTER ATLAS OF HUMANANATOMY
• Diagnostic Ultrasound Musculoskeletal
• FUNDAMENTALS OF MUSCULOSKELETAL ULTRASOUND
• IMAGING ANATOMY MUSCULOSKELETAL SECOND EDITION
• Radiopedia.