The document summarizes the peripheral nerves of the lower limb, focusing on the sciatic nerve and its branches. It discusses:
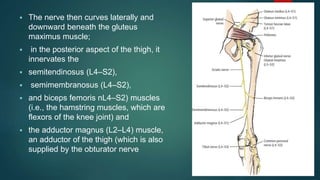
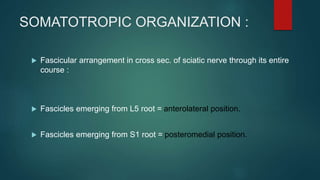
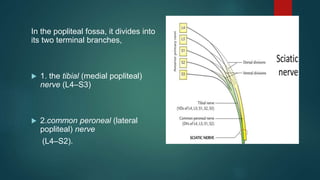
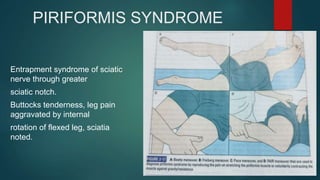
1) The sciatic nerve emerges from the sacral plexus and leaves the pelvis through the greater sciatic foramen. It divides in the popliteal fossa into the tibial and common peroneal nerves.
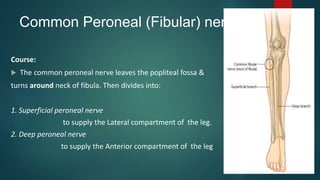
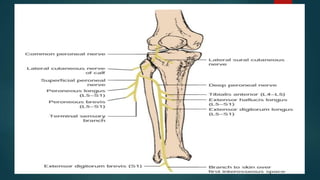
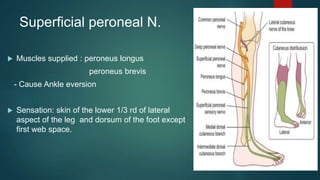
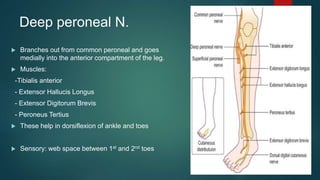
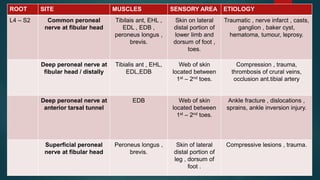
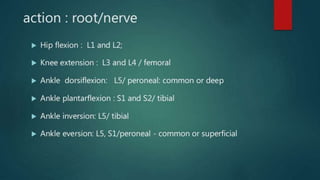
2) The common peroneal nerve divides into the superficial and deep peroneal nerves. The superficial nerve innervates muscles that cause ankle eversion while the deep nerve innervates muscles that cause dorsiflexion of the ankle and toes.
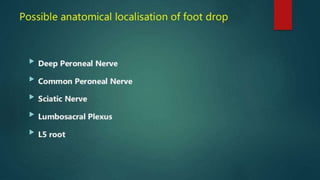
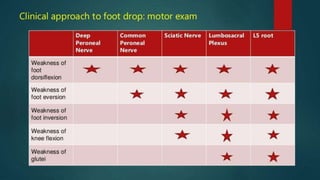
3) Injuries to the sciatic, common peroneal, and deep per



































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













