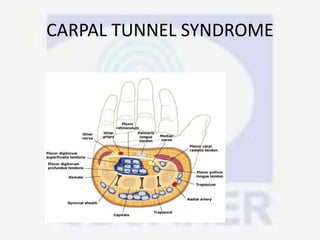
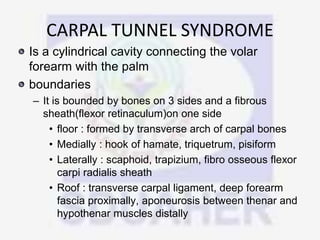
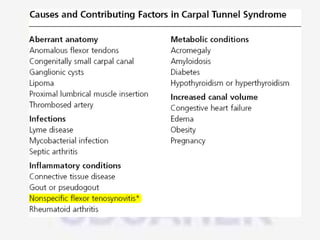
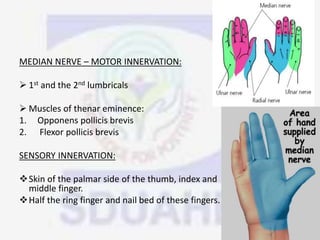
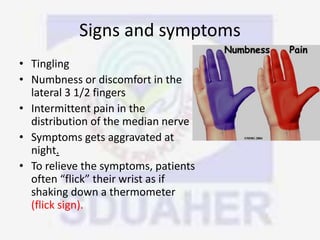
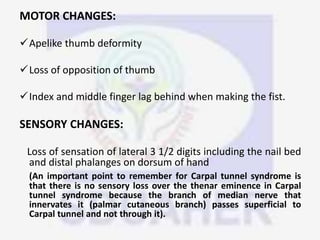
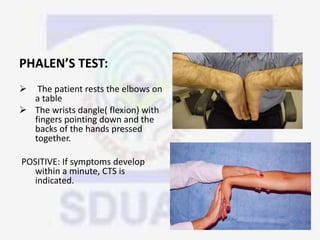
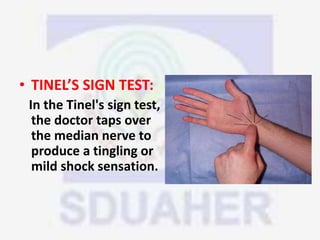
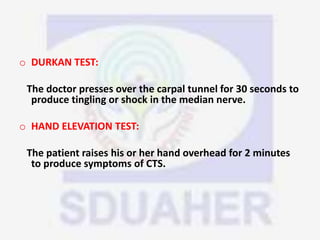
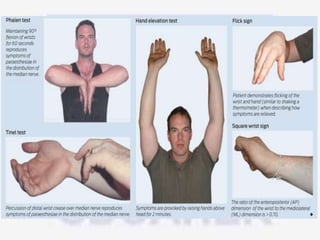
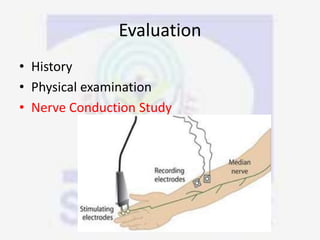
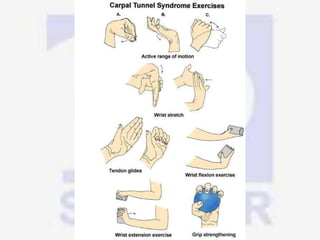
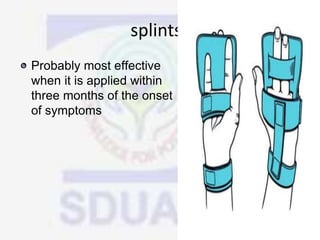
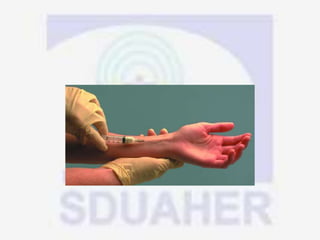
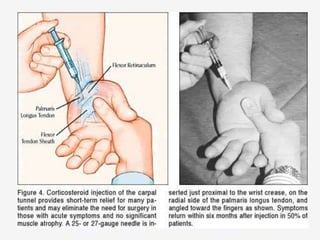
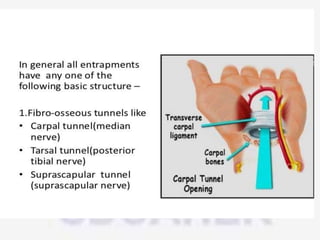
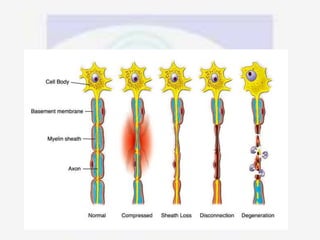
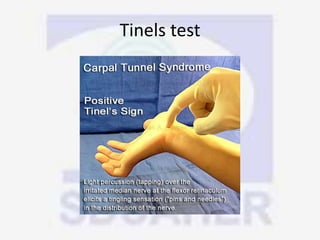
Nerve compression syndrome, also known as entrapment neuropathy, occurs when a peripheral nerve is compressed, causing mechanical damage. Carpal tunnel syndrome is a common example, where the median nerve is compressed as it passes through the carpal tunnel in the wrist. Symptoms include tingling, numbness, and pain in the fingers innervated by the median nerve that is worsened at night. Physical exams and tests like Phalen's maneuver, Tinel's sign, and nerve conduction studies can help diagnose CTS. Treatment involves splinting, medications, injections, or carpal tunnel release surgery if conservative measures fail.




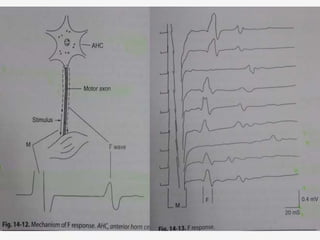
![• Properties of F waves:
• Latency, chronodispersion, amplitude,
persistence, F/M ratio, F estimation[ f
estimate = (2D/CV) X10 +1 +DL ]
• CLINICAL IMPORTANCE:
• Absent in sedated patient
• They study the entire course of nerve so they
are more reliable in neuropathies.](https://image.slidesharecdn.com/nervecompressionsyndrome-vaibhavmittal-170131063259/85/Nerve-compression-syndrome-37-320.jpg)