Downloaded 35 times


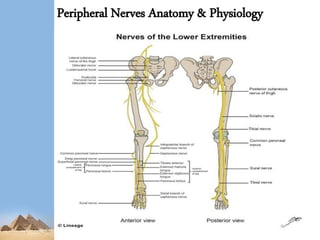

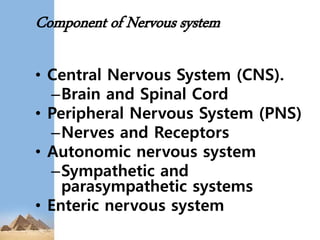

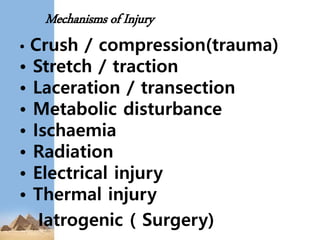















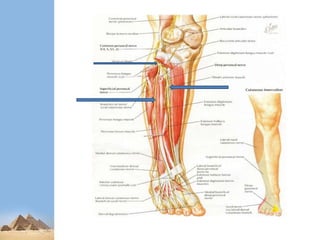














This presentation summarizes nerve injuries of the lower limb. It begins with an overview of the nervous system and its components. It then discusses the specific nerves of the lower limb, including their anatomy and areas of innervation. Various mechanisms of nerve injury are described. Sunderland and Seddon's classifications of nerve injuries are explained. Finally, the presentation covers assessment, investigations and management of nerve injuries, both conservative and surgical.






![Peripheral Nerves of Upper Limb [Radial, Median & Ulnar nerve]](https://cdn.slidesharecdn.com/ss_thumbnails/sb-190709091558-thumbnail.jpg?width=640&height=640&fit=bounds)




























































