Downloaded 4,119 times








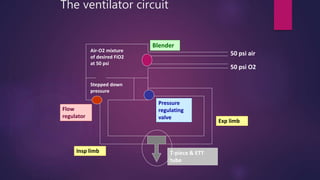
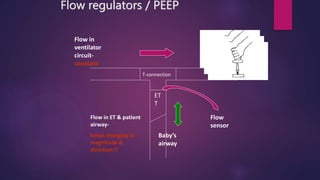
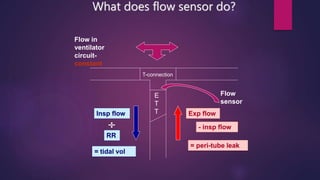


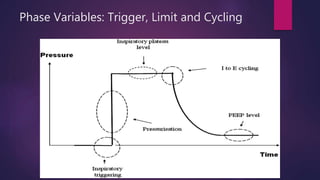
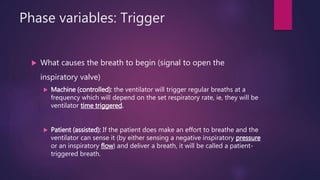



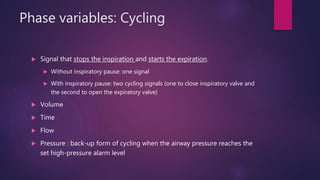
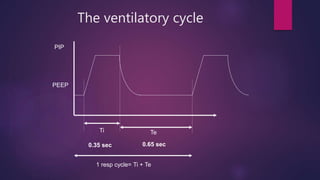
















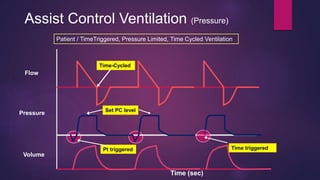
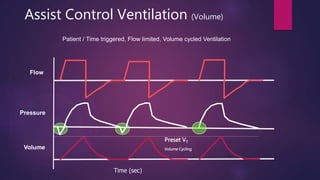
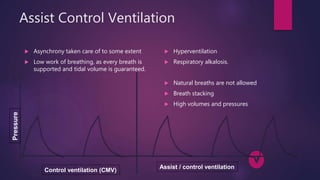
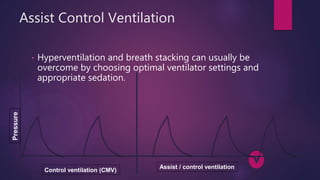
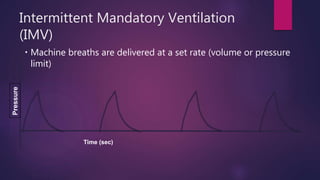
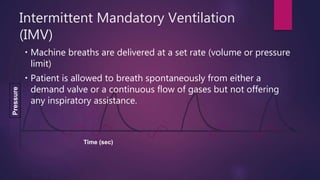









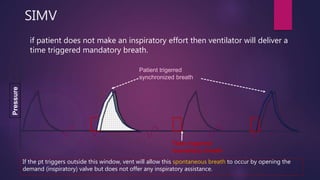
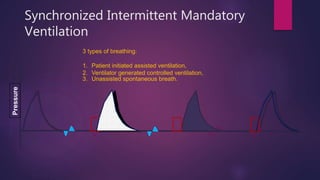
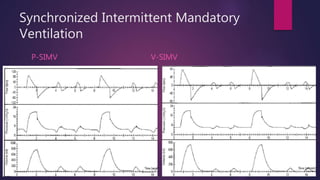











This document discusses various modes of mechanical ventilation. It begins by describing the basic components and functions of a ventilator. The document then explains the key parameters that ventilators can control including tidal volume, frequency, pressure, and time settings. Several common ventilation modes are described including controlled mandatory ventilation (CMV), assist-control ventilation, intermittent mandatory ventilation (IMV), and synchronized intermittent mandatory ventilation (SIMV). Each mode is defined by how the ventilator delivers breaths in terms of being time-triggered or patient-triggered and how breaths are cycled. The advantages and disadvantages of different modes are also briefly discussed.




















































































