Downloaded 945 times






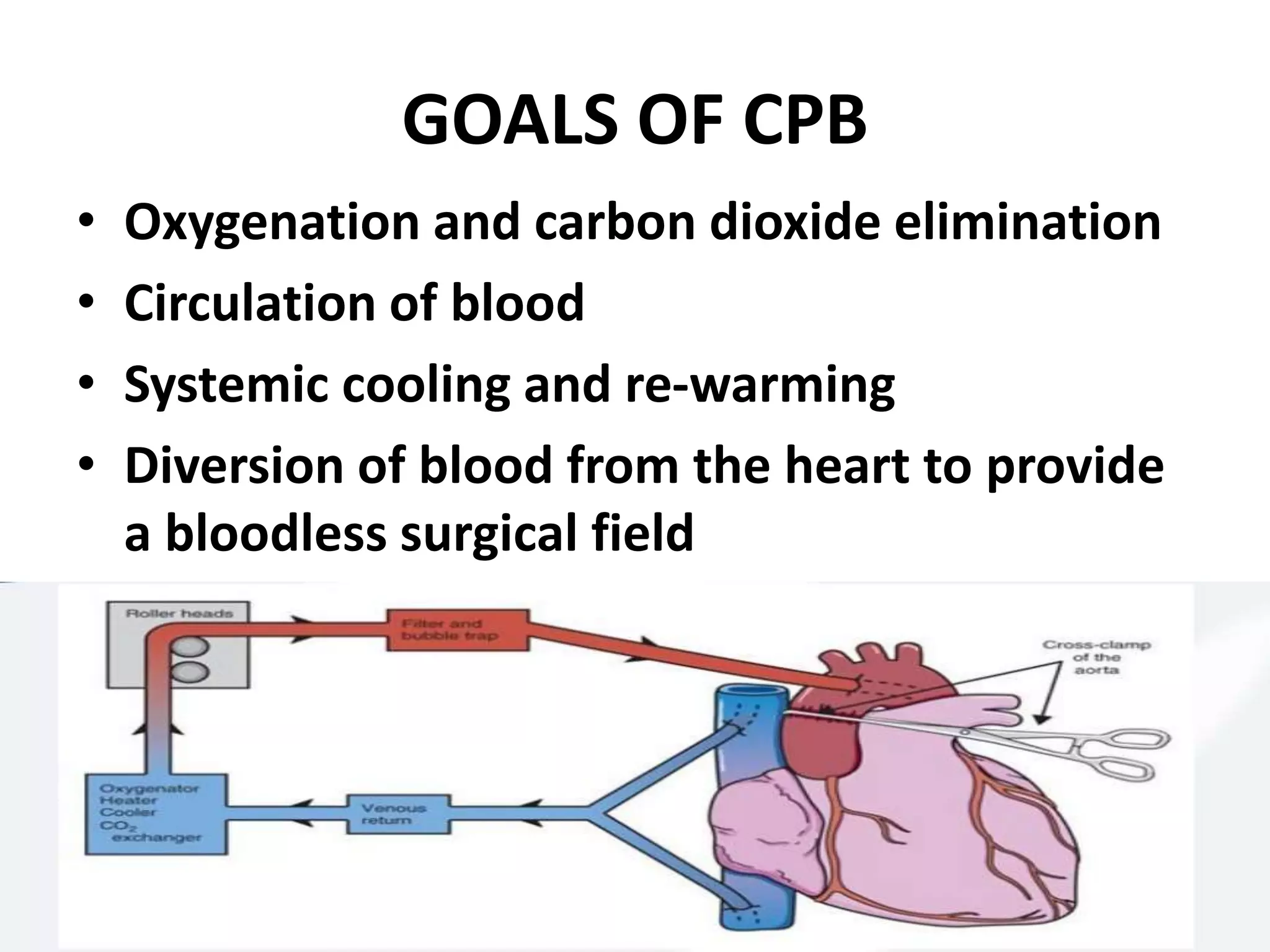
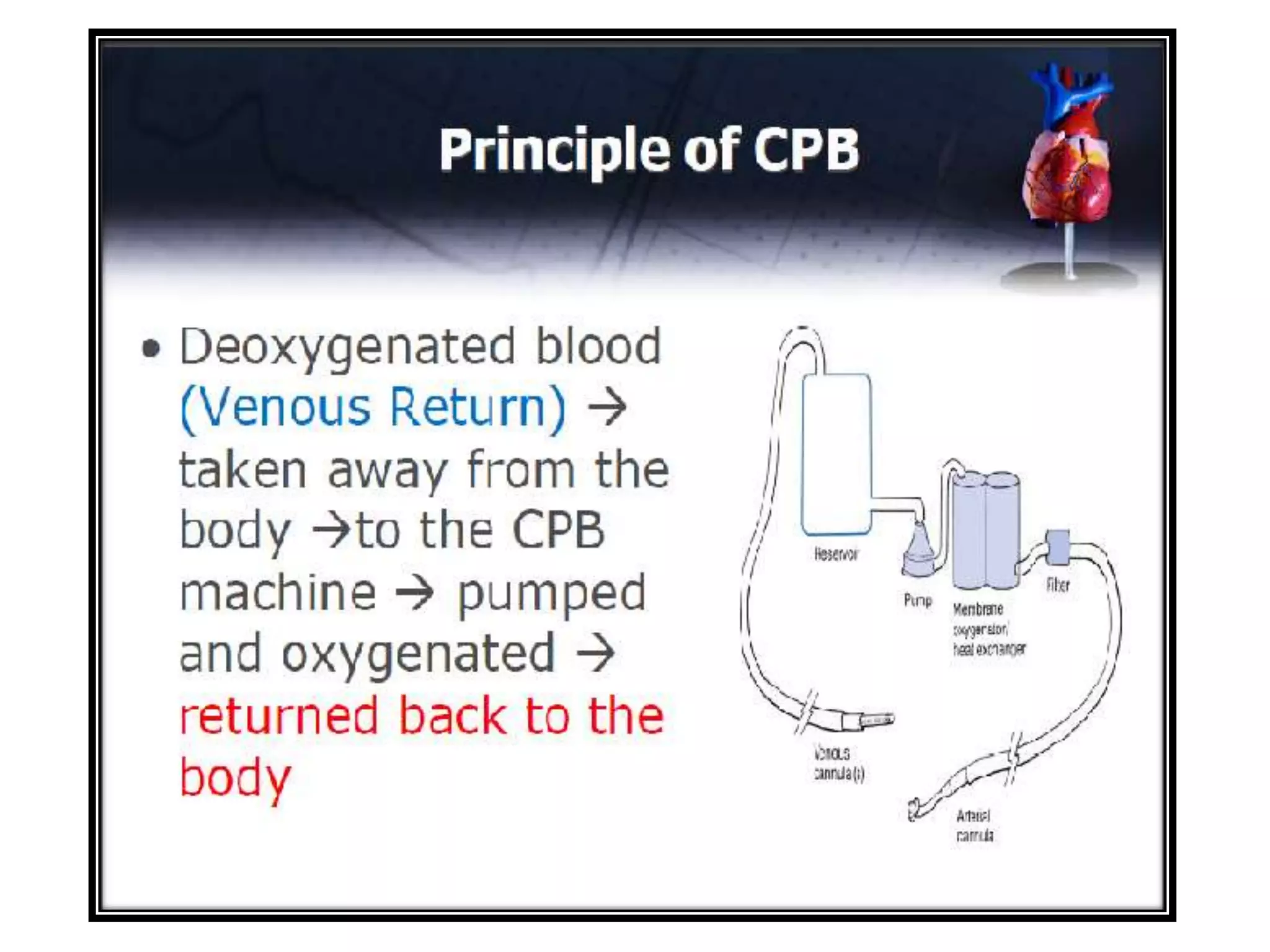











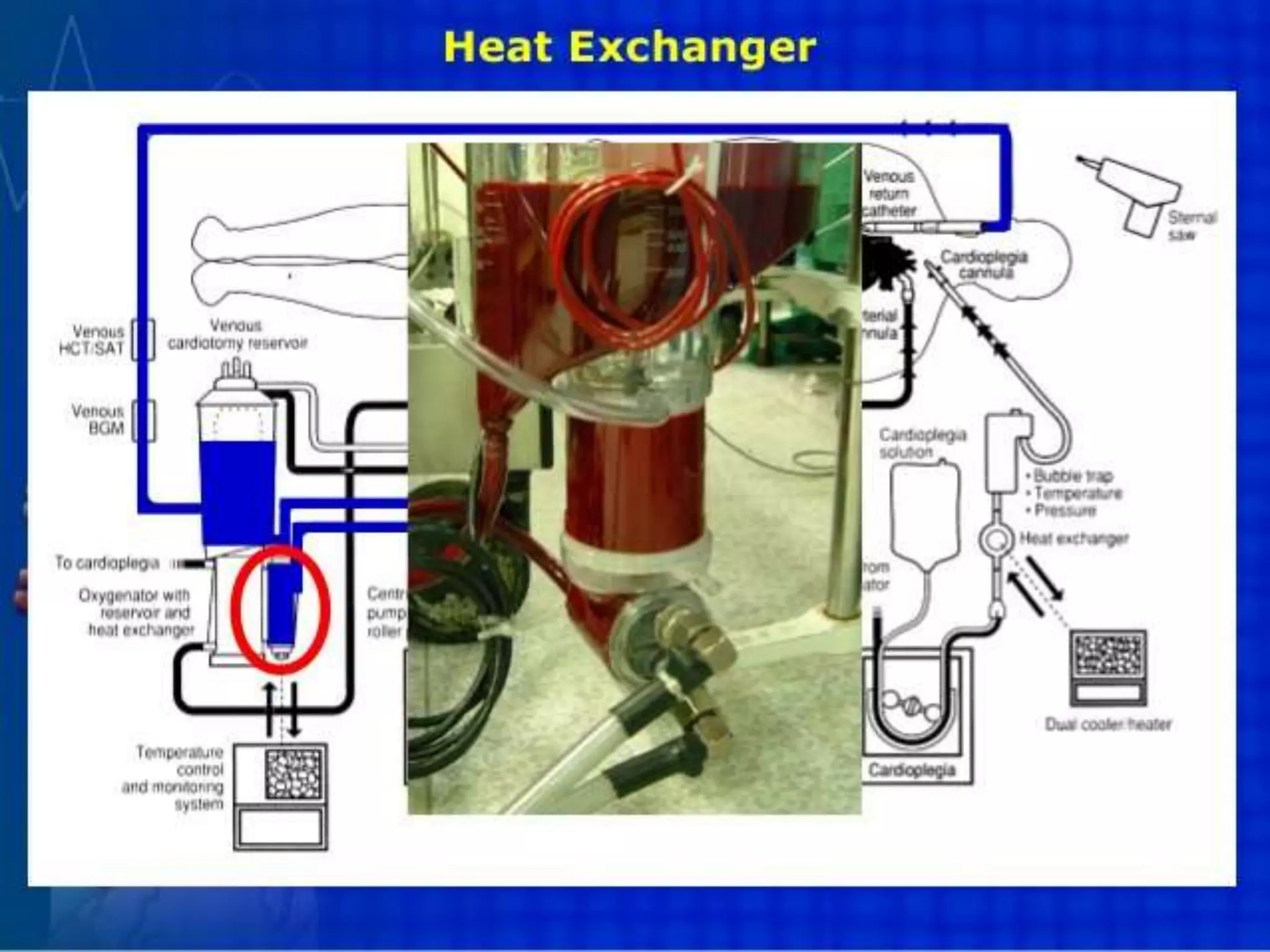



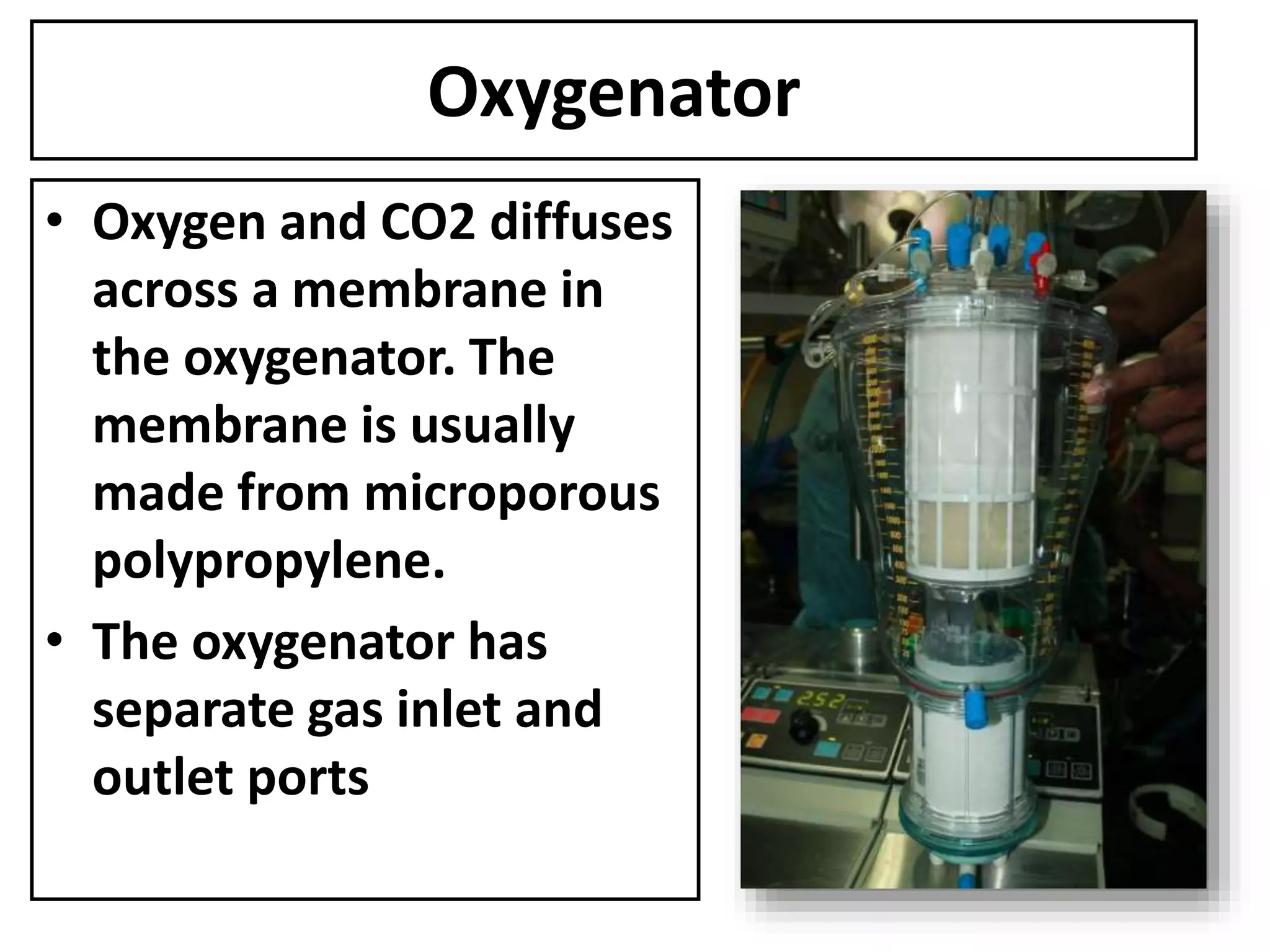

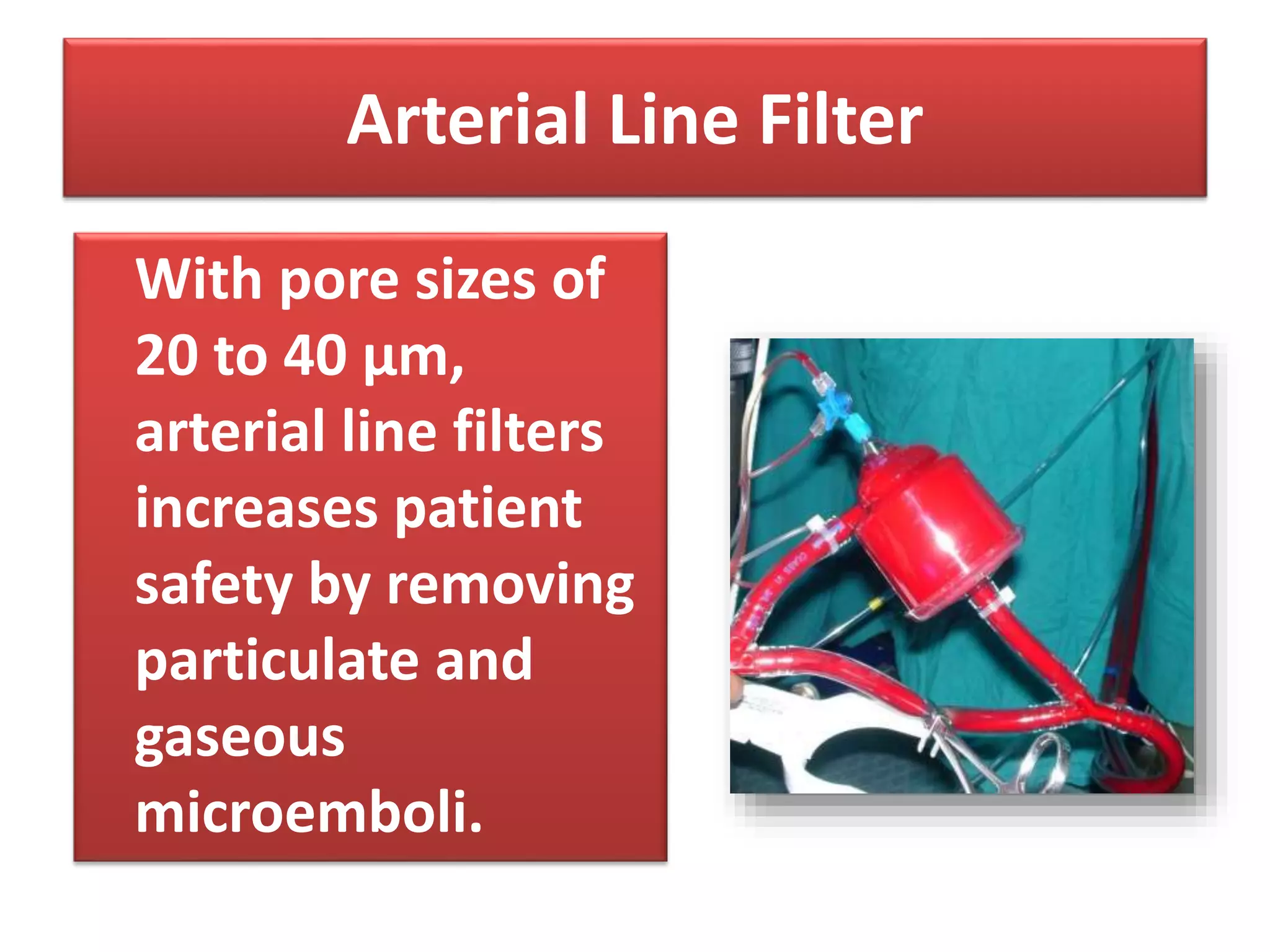
























This document provides information about cardiopulmonary bypass (CPB), including its goals, components, and processes. It discusses how CPB circuits divert blood flow away from the heart and lungs using a pump and oxygenator, allowing for surgery on a bloodless field. Key components that are described include the pump, oxygenator, heat exchanger, cannulas, and filters used. The document outlines the steps of priming, anticoagulation, cannulation, initiation and maintenance of bypass, as well as weaning and termination from bypass. Potential complications are also briefly mentioned.























































































