Downloaded 158 times

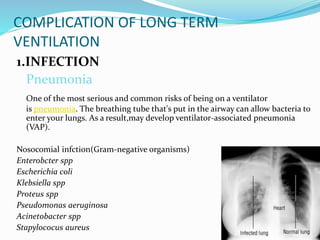
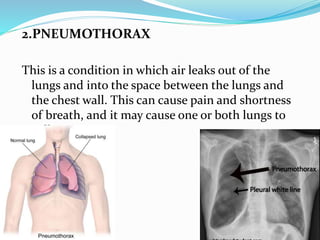



This document discusses mechanical ventilation and its complications. It begins by defining mechanical ventilation as assisted or controlled ventilation using mechanical devices. It then describes invasive mechanical ventilation, which uses an endotracheal or tracheostomy tube, and non-invasive ventilation without an artificial airway. Common indications for mechanical ventilation are then listed. The main body discusses complications of long-term ventilation, including infections like pneumonia, pneumothorax, injuries to the face and airway, gastrointestinal effects, renal effects, disrupted sleep, decubitus ulcers, malnutrition, depression/anxiety, and delirium.


































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
