











![Recommended Daily allowances
RDA
• The recommended daily intake of magnesium
varies by age and gender, but 400 mg is a good
round number for adults.
• The kidneys provide homeostasis, typically
excreting 120 mg/day.
• Since the 1960s, we have known that
consumption of alcohol, even in modest
amounts, can double or even quadruple the
excretion of magnesium.[1]
• Many over-the-counter and prescription drugs,
such as proton pump inhibitors, can lower body
magnesium levels.
Dr. Nandyala Venkateshwarlu
SVS Medical College](https://image.slidesharecdn.com/venkatmagnesium-150603154734-lva1-app6891/85/Venkat-magnesium-17-320.jpg)


![Some facts about prevalence
• There has been no large systematic study of the
adequacy of magnesium body stores in Americans.
• In 2009, the World Health Organization published a
report[2] that stated that 75% of Americans consumed
less magnesium than needed.
• Some say that we have a nationwide magnesium
deficiency.
• Certainly, those named illnesses are common.
Obviously, the National Institutes of Health or the
Centers for Disease Control and Prevention should fund
serious work to ascertain the status of Americans'
magnesium body stores.
Dr. Nandyala Venkateshwarlu
SVS Medical College](https://image.slidesharecdn.com/venkatmagnesium-150603154734-lva1-app6891/85/Venkat-magnesium-20-320.jpg)





























![Clinical features
• Magnesium deficiency has been blamed for
various arrhythmias, hypertension, attention-
deficit/hyperactivity disorder, anxiety,
seizures, leg cramps, restless legs syndrome,
kidney stones, myocardial infarction,
headaches, premenstrual syndrome,
fibromyalgia, chest pain, osteoporosis,
altitude sickness, diabetes, fatigue, weakness,
and other maladies.[1]
Dr. Nandyala Venkateshwarlu
SVS Medical College](https://image.slidesharecdn.com/venkatmagnesium-150603154734-lva1-app6891/85/Venkat-magnesium-50-320.jpg)





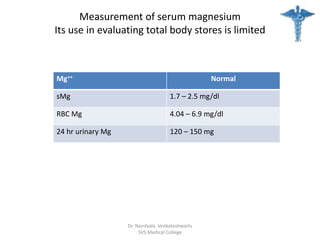


![Excretion Analysis
FEMg = [(UMg x PCr) / (PMg x UCr x 0.7)]
• Distinction between gastrointestinal and renal losses
can be made by measuring the 24-hour urinary
magnesium excretion or the FE of magnesium on a
random urine specimen
• Daily excretion of more than 24 mg or calculated FE of
magnesium above 3% in a subject with normal renal
function indicates renal magnesium wasting.
Dr. Nandyala Venkateshwarlu
SVS Medical College](https://image.slidesharecdn.com/venkatmagnesium-150603154734-lva1-app6891/85/Venkat-magnesium-60-320.jpg)


























![Cardiovascular abnormality
• Magnesium is an effective calcium channel
blocker both extracellularly and intracellularly; in
addition, intracellular magnesium profoundly
blocks several cardiac potassium channels [1].
These changes can combine to impair
cardiovascular function
• ECG Changes: prolongation of the P-R interval, an
increase in QRS duration, and an increase in Q-T
interval. Complete heart block and cardiac arrest
may occur at a plasma magnesium concentration
above 15 meq/L.
Dr. Nandyala Venkateshwarlu
SVS Medical College](https://image.slidesharecdn.com/venkatmagnesium-150603154734-lva1-app6891/85/Venkat-magnesium-87-320.jpg)








Magnesium is the eighth most abundant element in the Earth's crust and plays crucial roles in various bodily functions, including blood pressure regulation and biochemical reactions. It is primarily absorbed in the jejunum and ileum, with dietary sources including green vegetables, nuts, and whole grains, requiring an intake of about 400 mg for adults. Hypomagnesaemia may arise from inadequate intake, increased renal excretion, or gastrointestinal losses, with significant implications for health, particularly among certain populations.






























![Magnesium [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/magnesiumautosaved-140828145928-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
























































