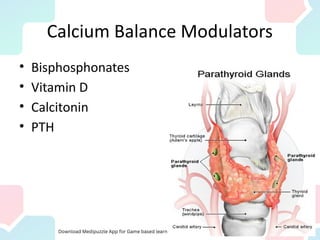
The document discusses the significance of calcium balance, including its physiological roles and the various disorders associated with its imbalance such as hypercalcemia and osteoporosis. It outlines the physiology of calcium absorption, excretion, and the effects of drugs like bisphosphonates and vitamin D on calcium metabolism. The regulatory mechanisms involving calcitonin and parathyroid hormone are also explained, highlighting their importance in maintaining calcium homeostasis.