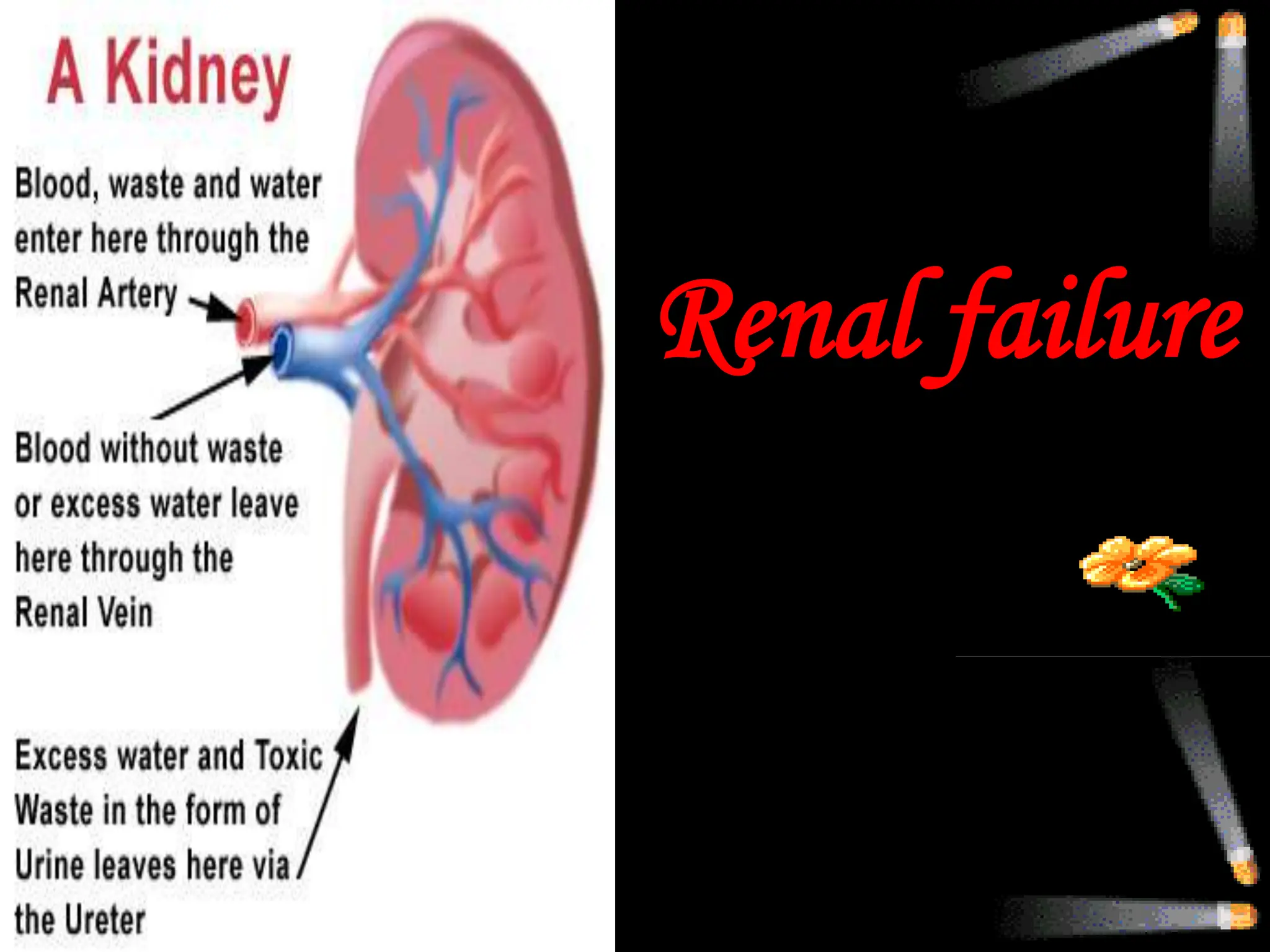
Renal failure occurs when the kidneys cannot remove waste or regulate fluids and electrolytes. There are two main types: acute renal failure, which develops rapidly over hours to days; and chronic renal failure, which is progressive and irreversible. Acute renal failure causes a sudden loss of kidney function and can result from prerenal issues, direct kidney damage, or urinary tract obstruction. Chronic renal failure is treated through diet, medication, and often dialysis to remove waste when kidney function declines. Nursing focuses on managing complications, nutrition, fluid balance, and educating patients.