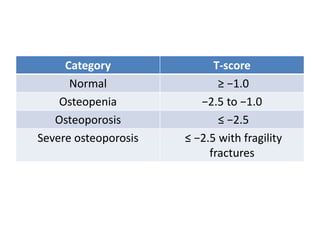
This document discusses osteoporosis and osteoporosis drugs. It defines osteoporosis and describes methods of diagnosis. It lists risk factors and medical conditions that can lead to osteoporosis. It then discusses several classes of drugs used to treat osteoporosis, including bisphosphonates, calcium, vitamin D, calcitonin, teriparatide, vitamin K2, strontium ranelate, denosumab, and raloxifene. For each drug, it provides information on mechanisms of action, dosages, formulations, and side effects.