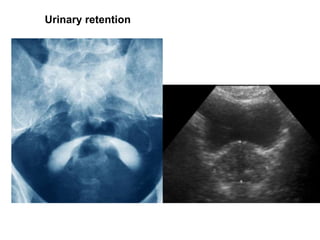
This document discusses trauma to the urinary tract and genitals. It covers kidney trauma, which is classified into 5 grades based on severity of injury. It also discusses ureteral injuries, which are classified into 5 grades. Urinary bladder trauma can be open, closed, or iatrogenic and can be intraperitoneal or extraperitoneal. Urethral injuries are discussed as well as external genital trauma including injuries to the penis, scrotum, testes and epididymis. Diagnostic tools like ultrasound, CT scans, and retrograde urethrography are covered. Treatment depends on the severity and includes both conservative and surgical approaches.