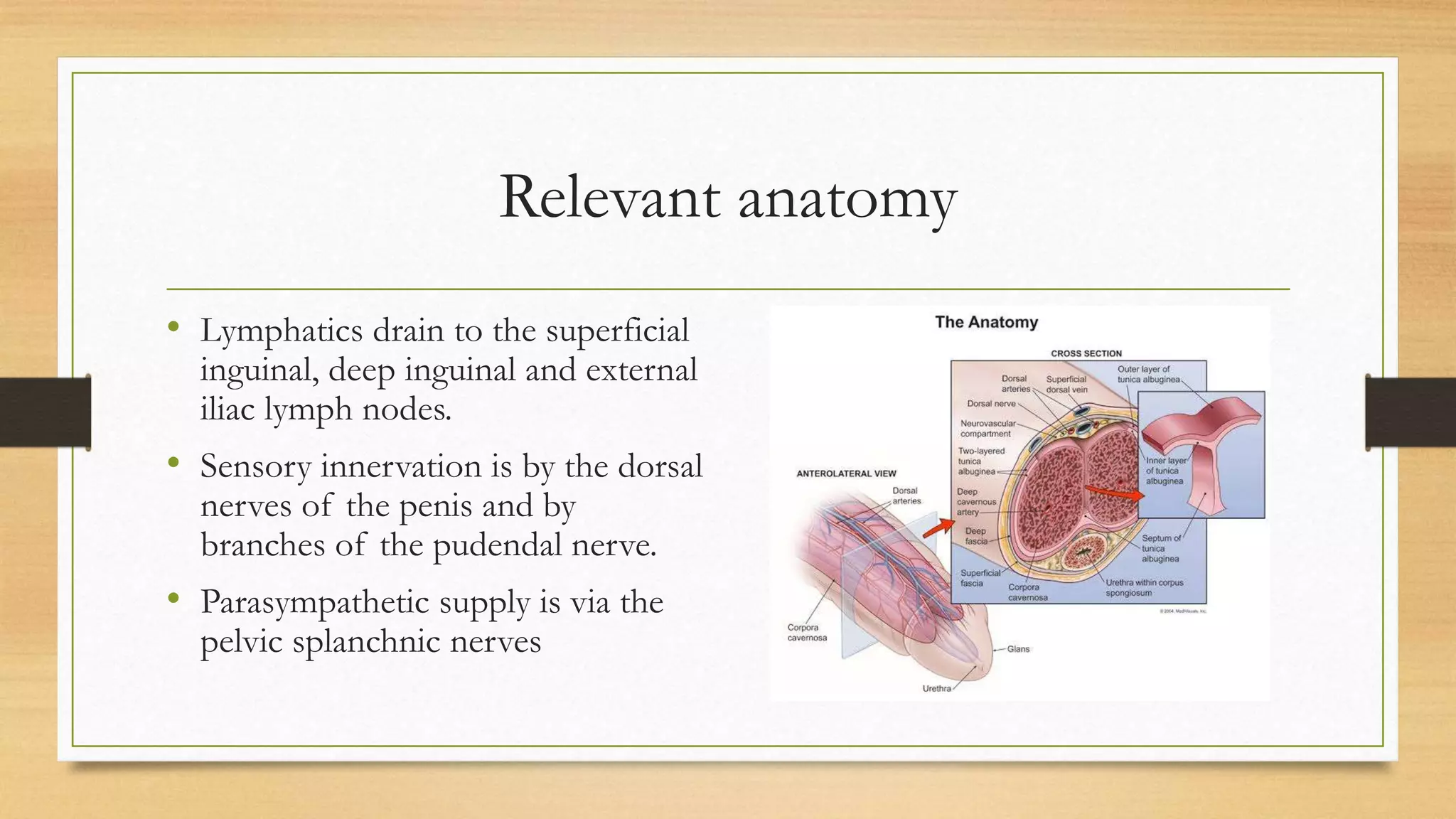
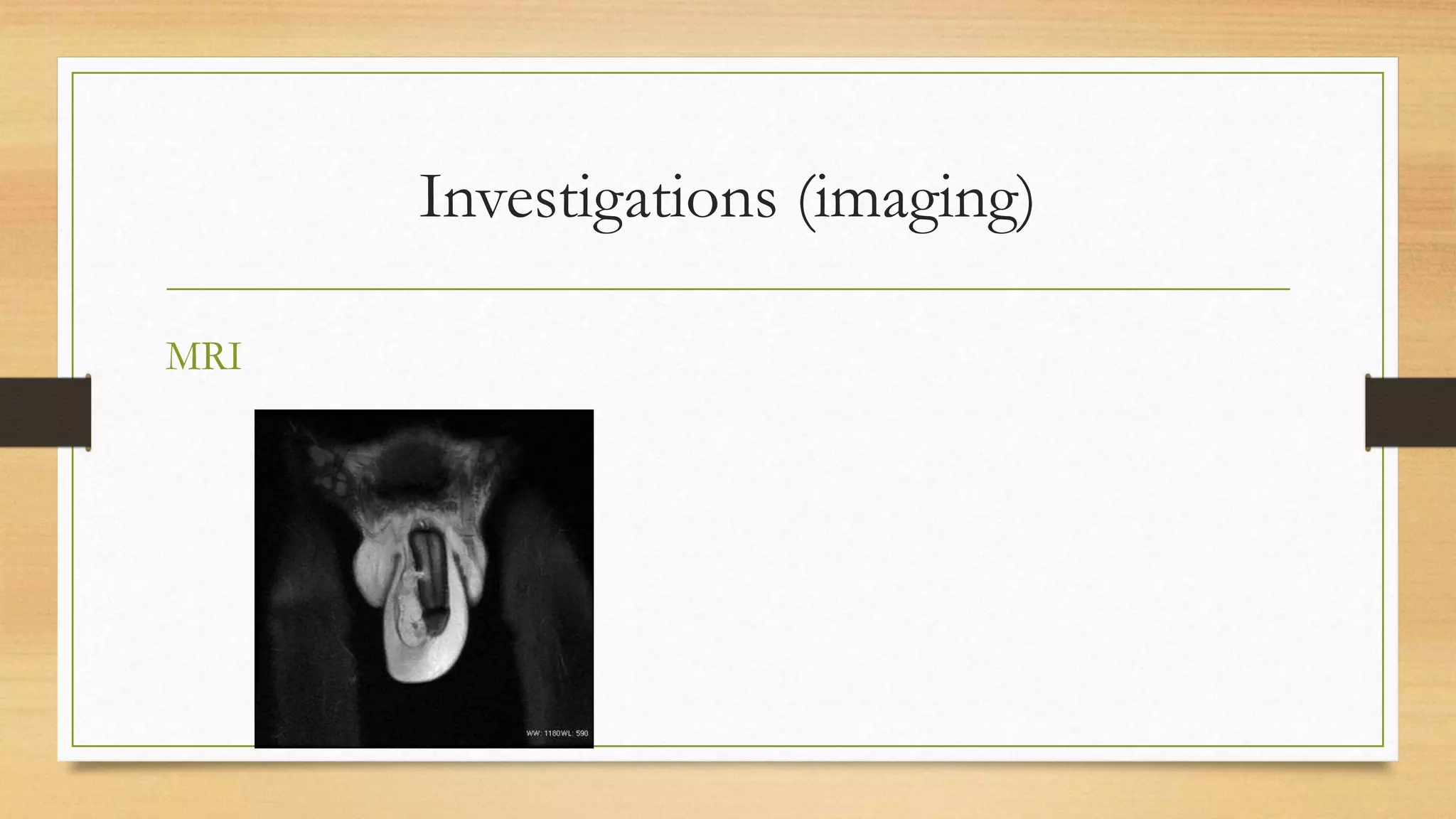
This document provides an overview of penile fracture, including relevant anatomy, causes, clinical presentation, diagnosis, treatment options, and postoperative care. It begins with an outline of the topics covered. The main points are: penile fracture involves a rupture of the corpus cavernosum during erection, most common causes are sexual intercourse and trauma from bending, patients experience pain, swelling and detumescence, diagnosis is usually clinical but imaging can help, and surgical repair within 24 hours has the best outcomes and aims to repair tears while preventing erectile dysfunction and abnormal healing.