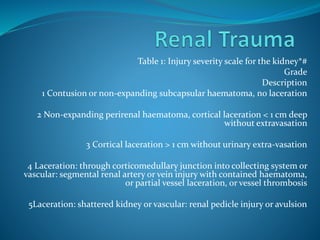
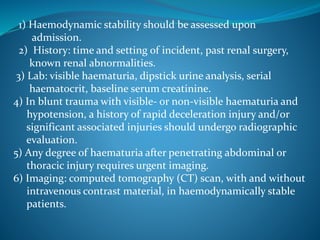
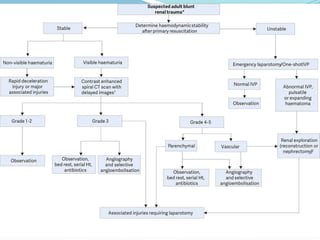
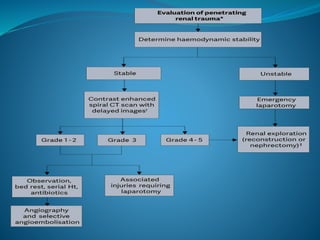
The document describes injury scales for the kidney and outlines the diagnostic evaluation and management of various genitourinary traumas, including kidney injuries, ureteral trauma, bladder trauma, urethral trauma, and penile fracture. It provides grading scales for kidney injuries and outlines recommended diagnostic imaging tests and surgical or conservative treatment approaches for different types and severities of genitourinary injuries.