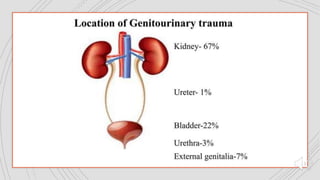
This document discusses various types of genitourinary trauma, including renal, bladder, ureteral, and scrotal trauma. It provides details on the mechanisms, classifications, imaging findings, and treatment approaches for each type of injury. Radiology plays an important role in accurately diagnosing and grading genitourinary trauma in order to guide clinical management decisions. CT is often the preferred imaging modality due to its ability to simultaneously evaluate the kidneys, bladder, and other abdominal organs.