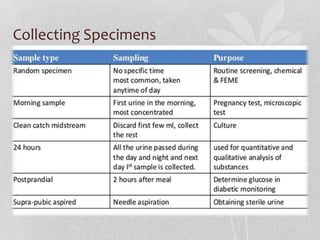
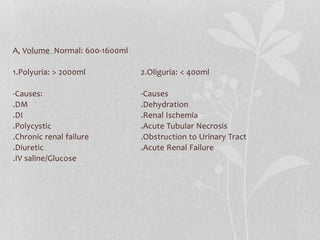
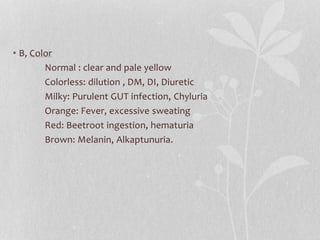
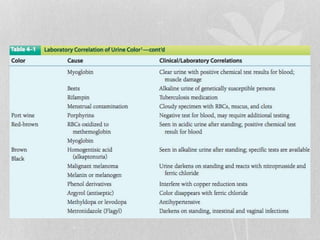
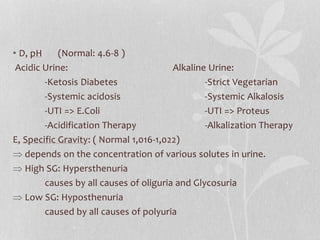
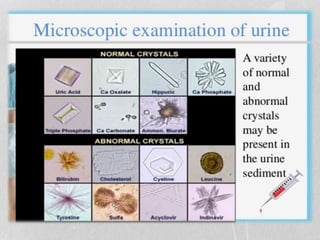
Urine analysis is a common medical diagnostic tool that can evaluate general health, diagnose diseases of the kidneys and urinary tract, and monitor conditions like diabetes. A urine analysis involves macroscopic examination of properties like volume, color, odor, pH and specific gravity. Microscopic examination analyzes cellular elements and crystals in sediment. Chemical analysis tests for proteins, glucose, ketones, blood, and other substances. Abnormal results can indicate issues with the kidneys, urinary tract, liver or other organs. Precise diagnosis requires correlating clinical history with comprehensive urine analysis findings.