Downloaded 141 times












![Causes
The main cause of TB is Mycobacterium tuberculosis, a
small, aerobic, nonmotile bacillus.[10] The
high lipid content of this pathogen accounts for many of
its unique clinical characteristics.[19] It divides every 16
to 20 hours, which is an extremely slow rate compared
with other bacteria, which usually divide in less than an
hour.[20] Mycobacteria have an outer membrane lipid
bilayer.
MTB can withstand weak disinfectants and survive in
a dry state for weeks. In nature, the bacterium can
grow only within the cells of a host organism, but M.
tuberculosis can be cultured in the laboratory](https://image.slidesharecdn.com/tuberculosis-141211002753-conversion-gate01/85/Classification-and-prophylactics-of-tuberculosis-24-320.jpg)






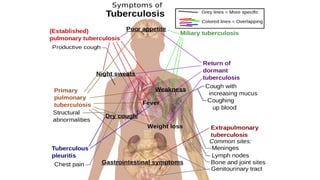
Tuberculosis is a widespread infectious disease caused by mycobacteria that typically affects the lungs. It spreads through airborne droplets when infected people cough, sneeze or speak. Symptoms include fever, night sweats, and weight loss. While most infections are latent and asymptomatic, active disease can be fatal if left untreated. Tuberculosis is treated with a combination of antibiotics taken for at least six months.











































































