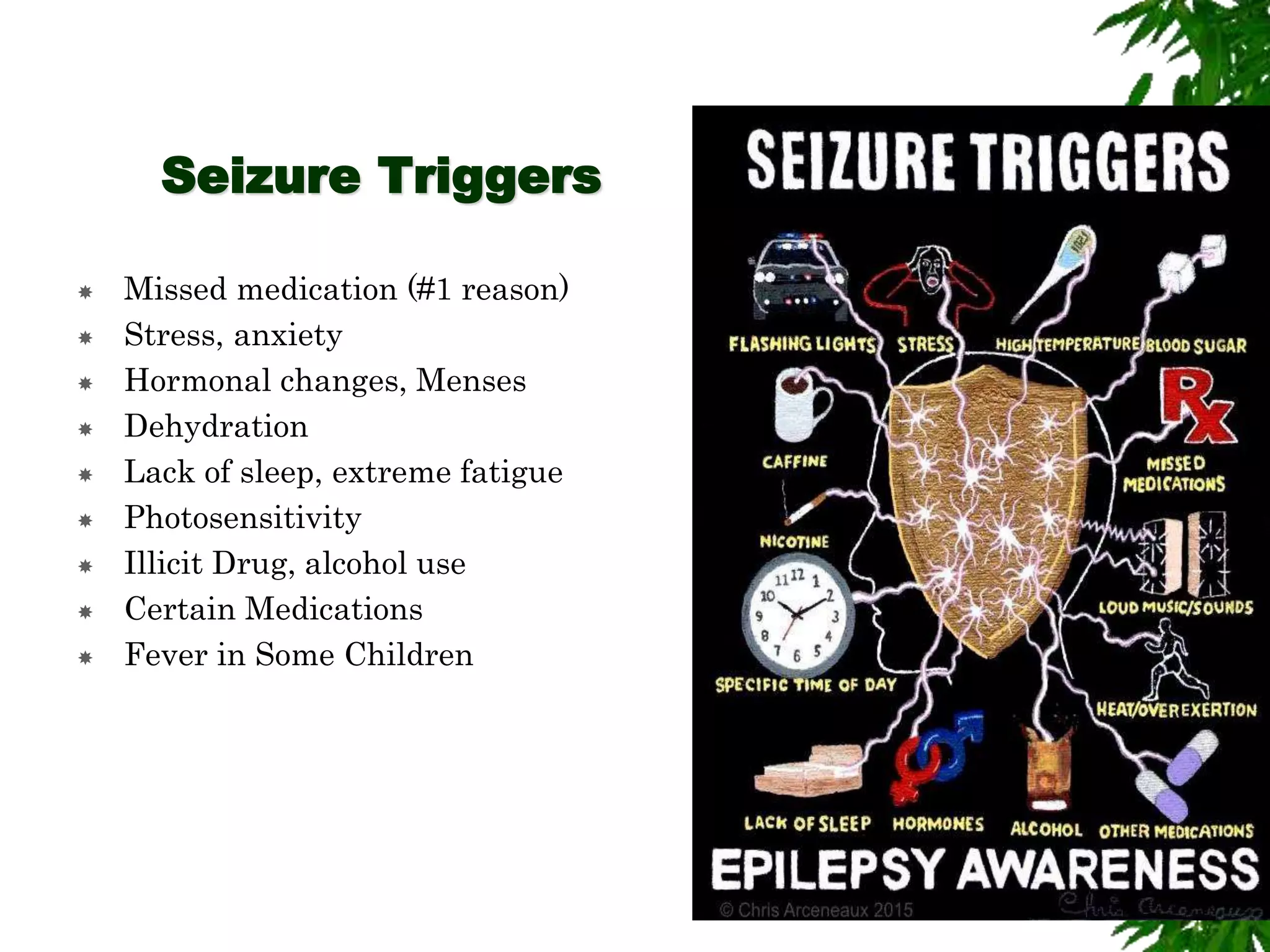
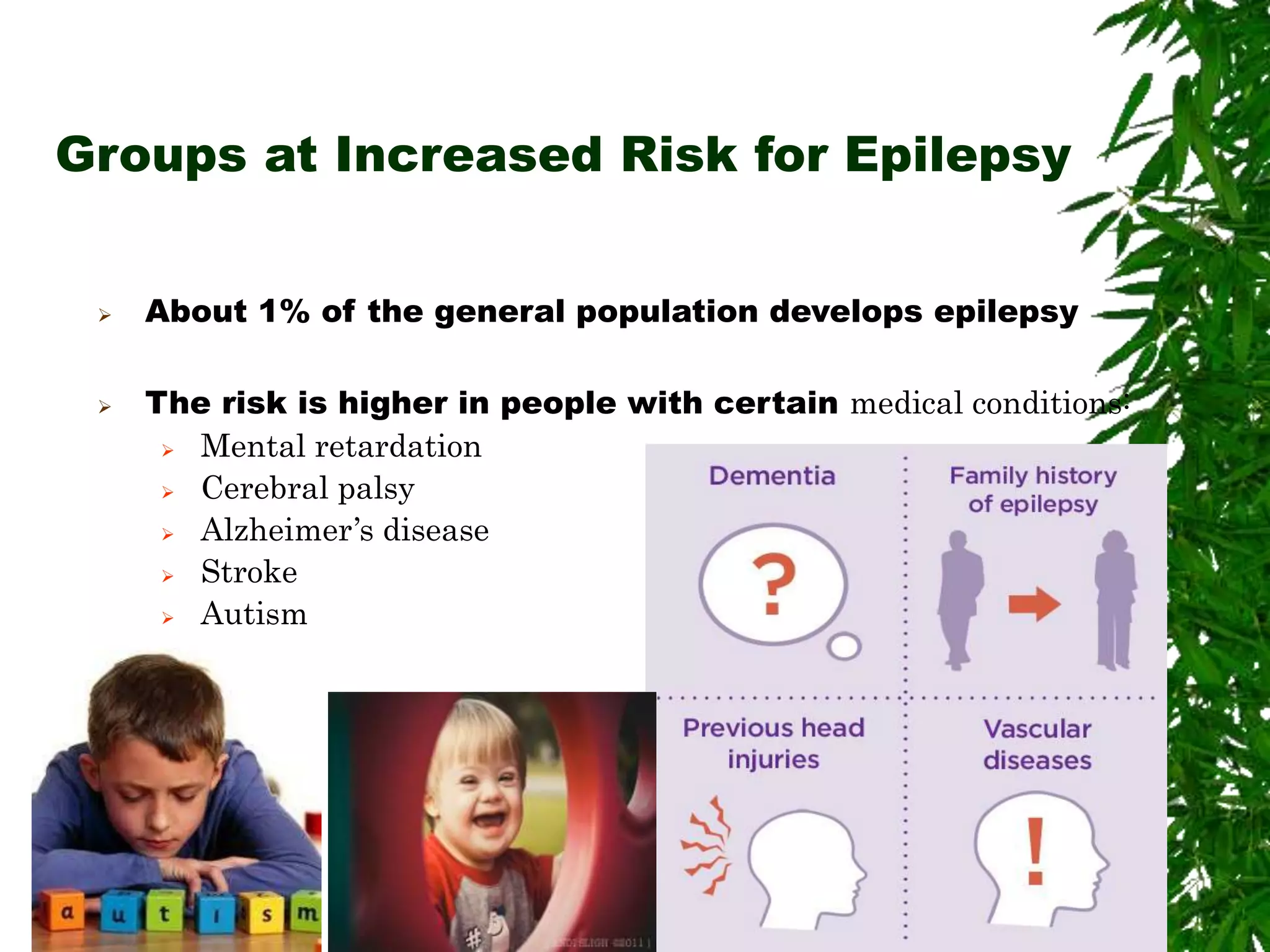
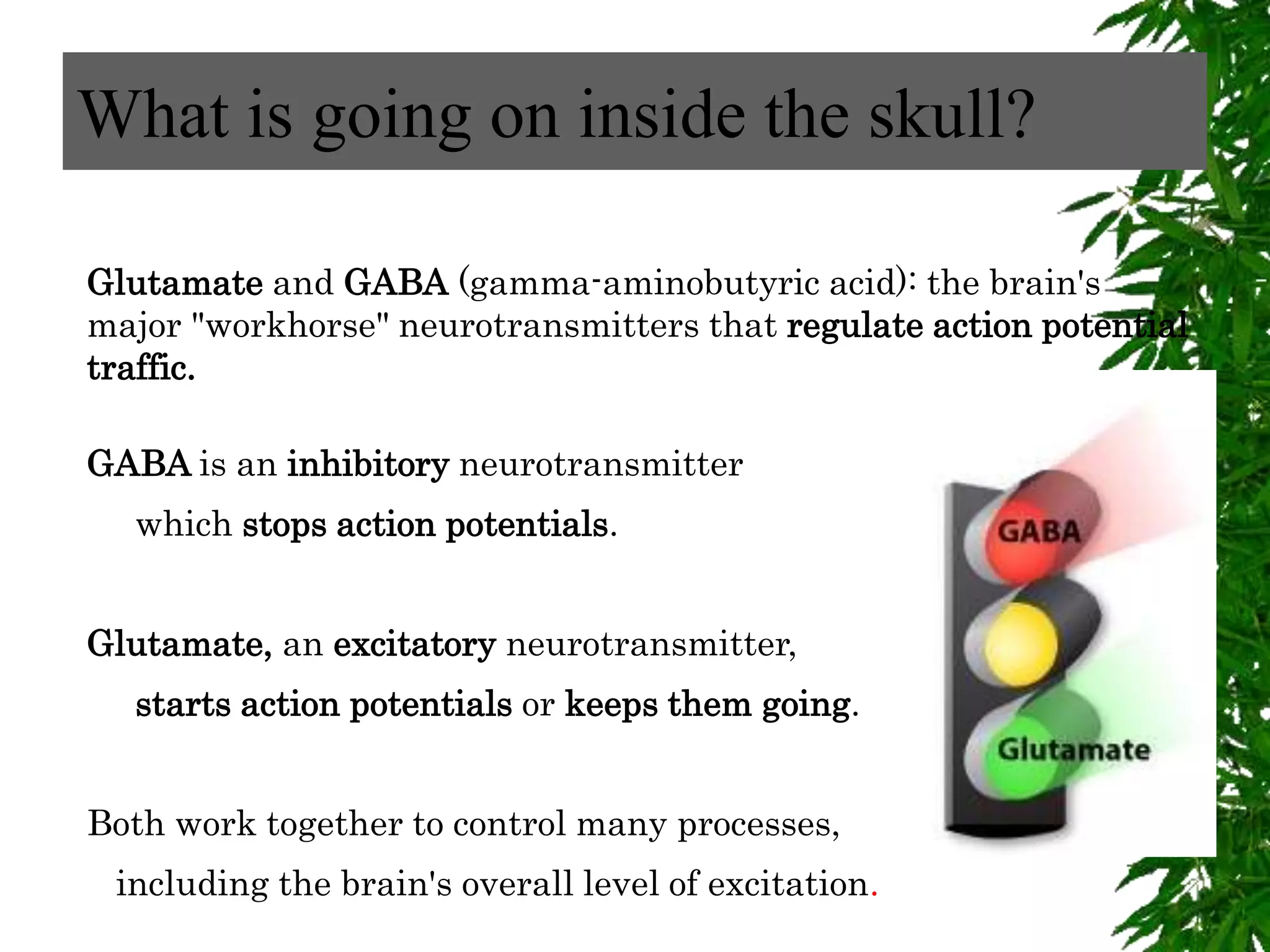
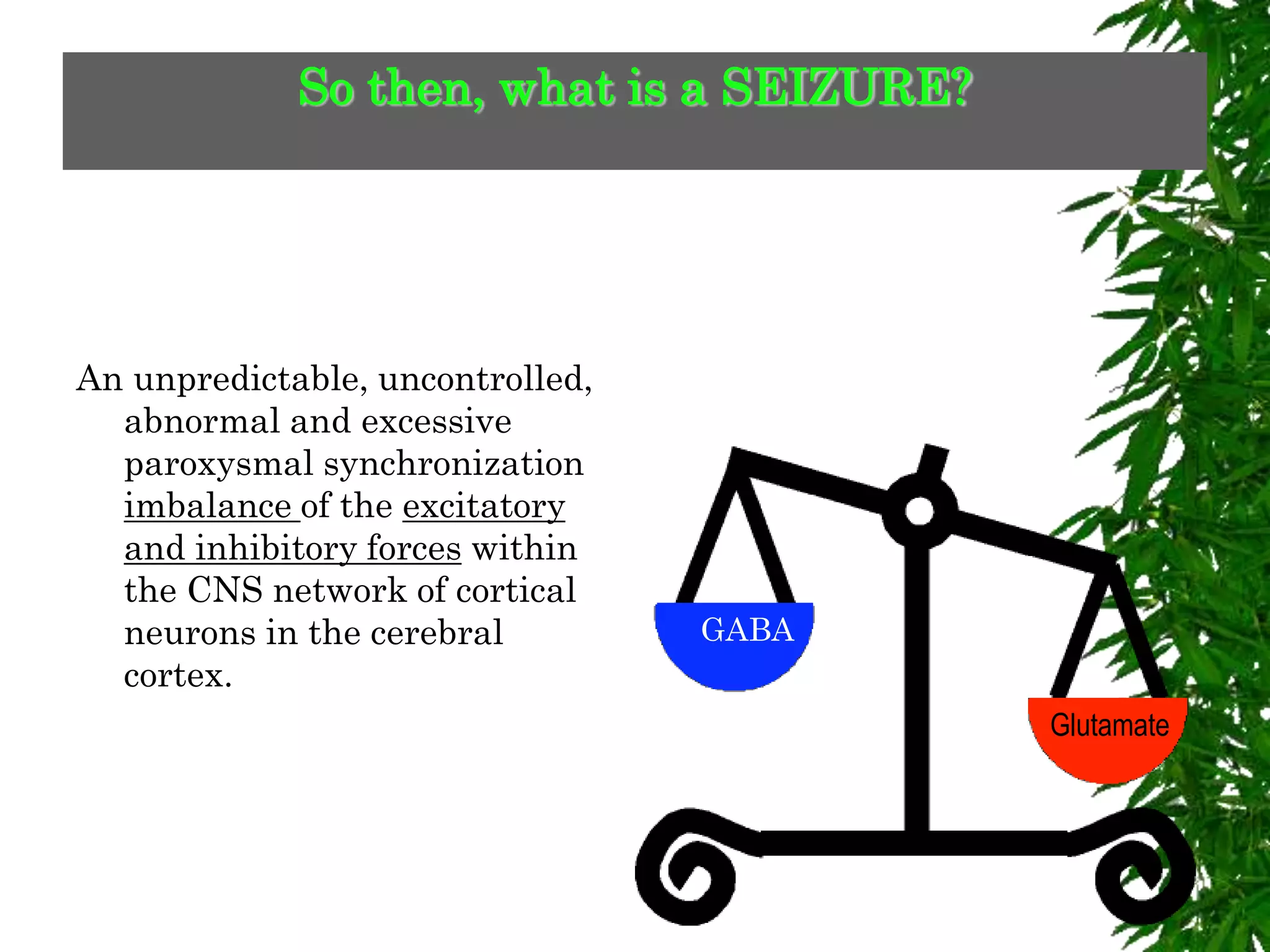
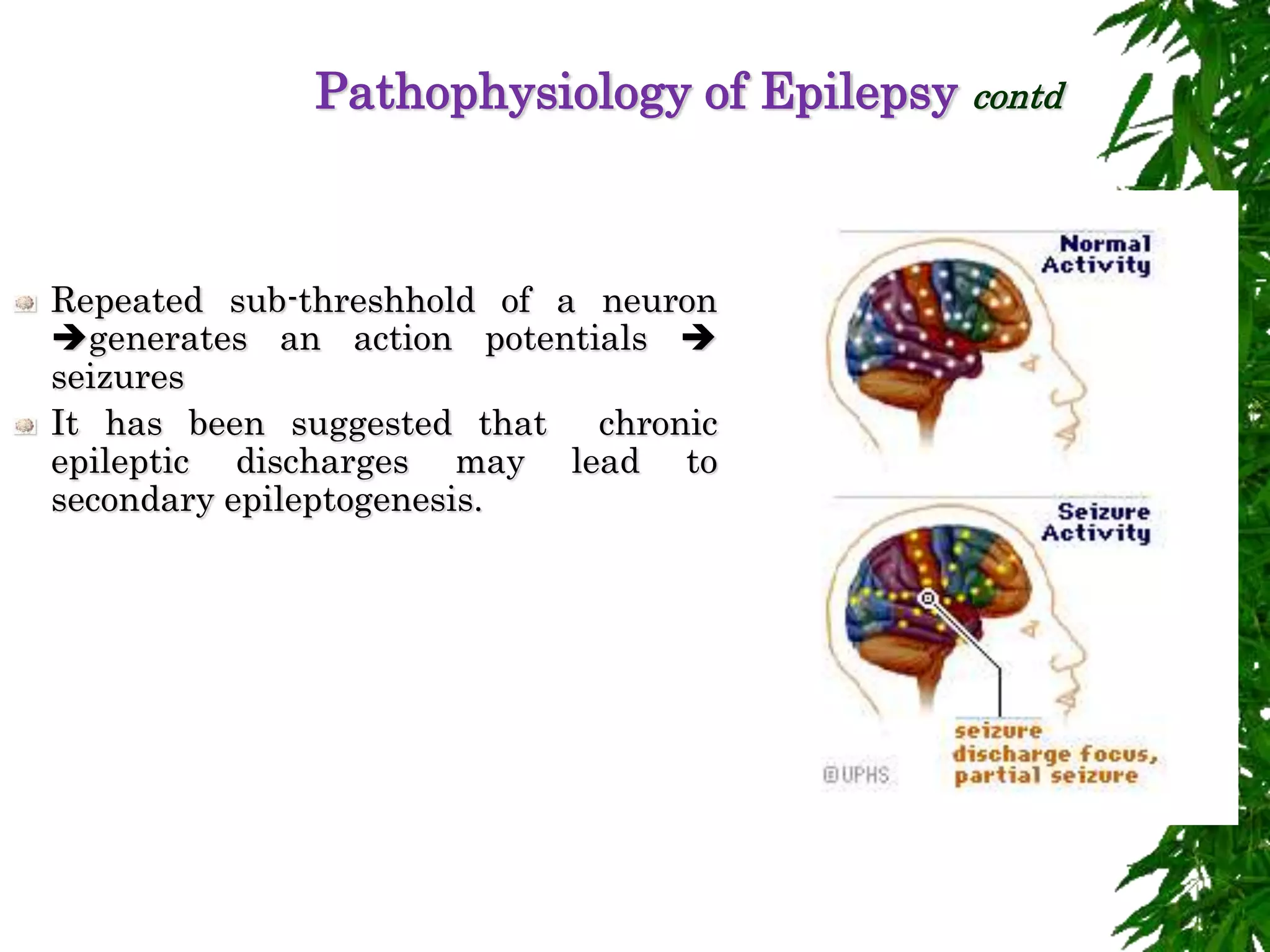
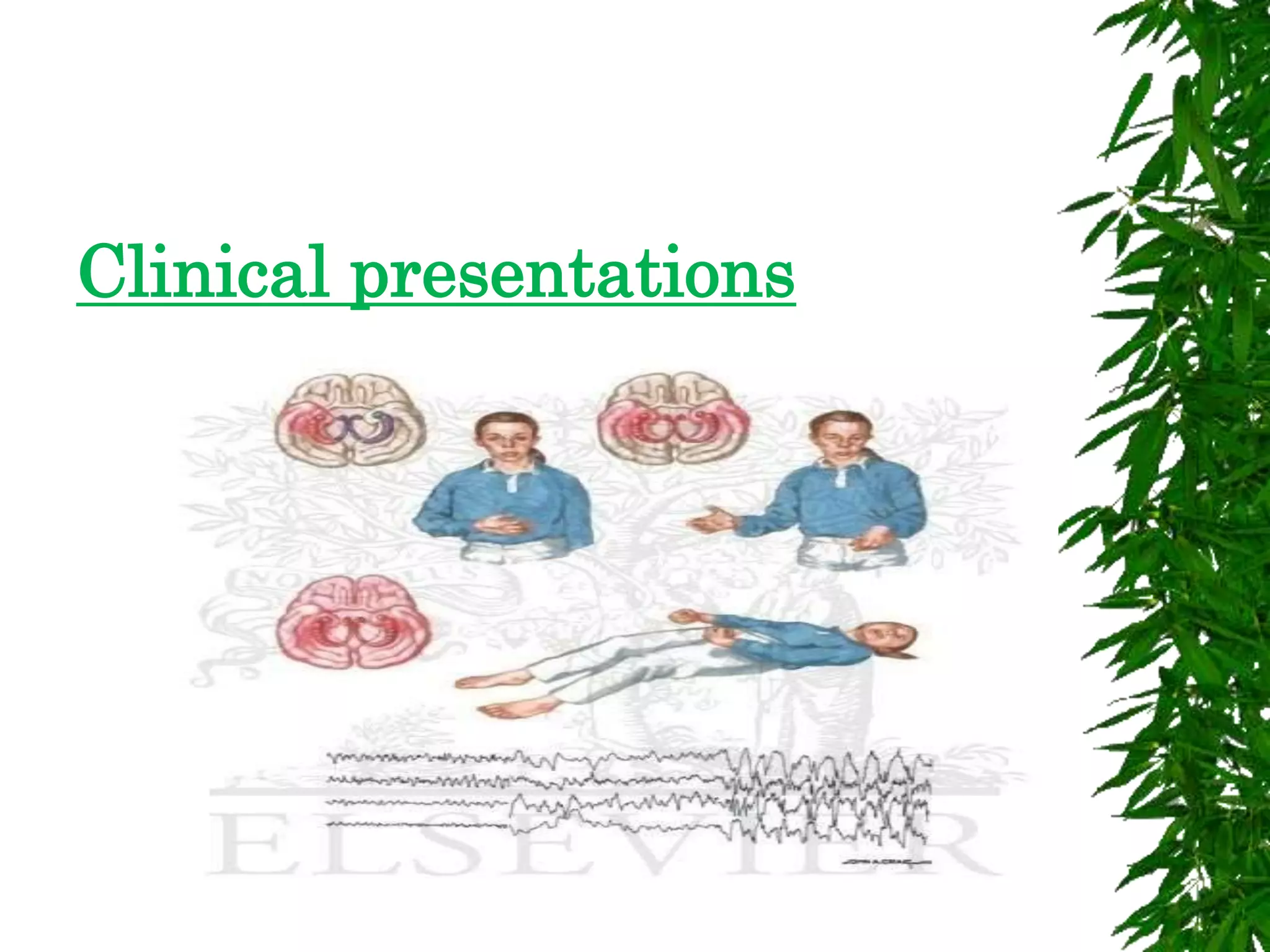
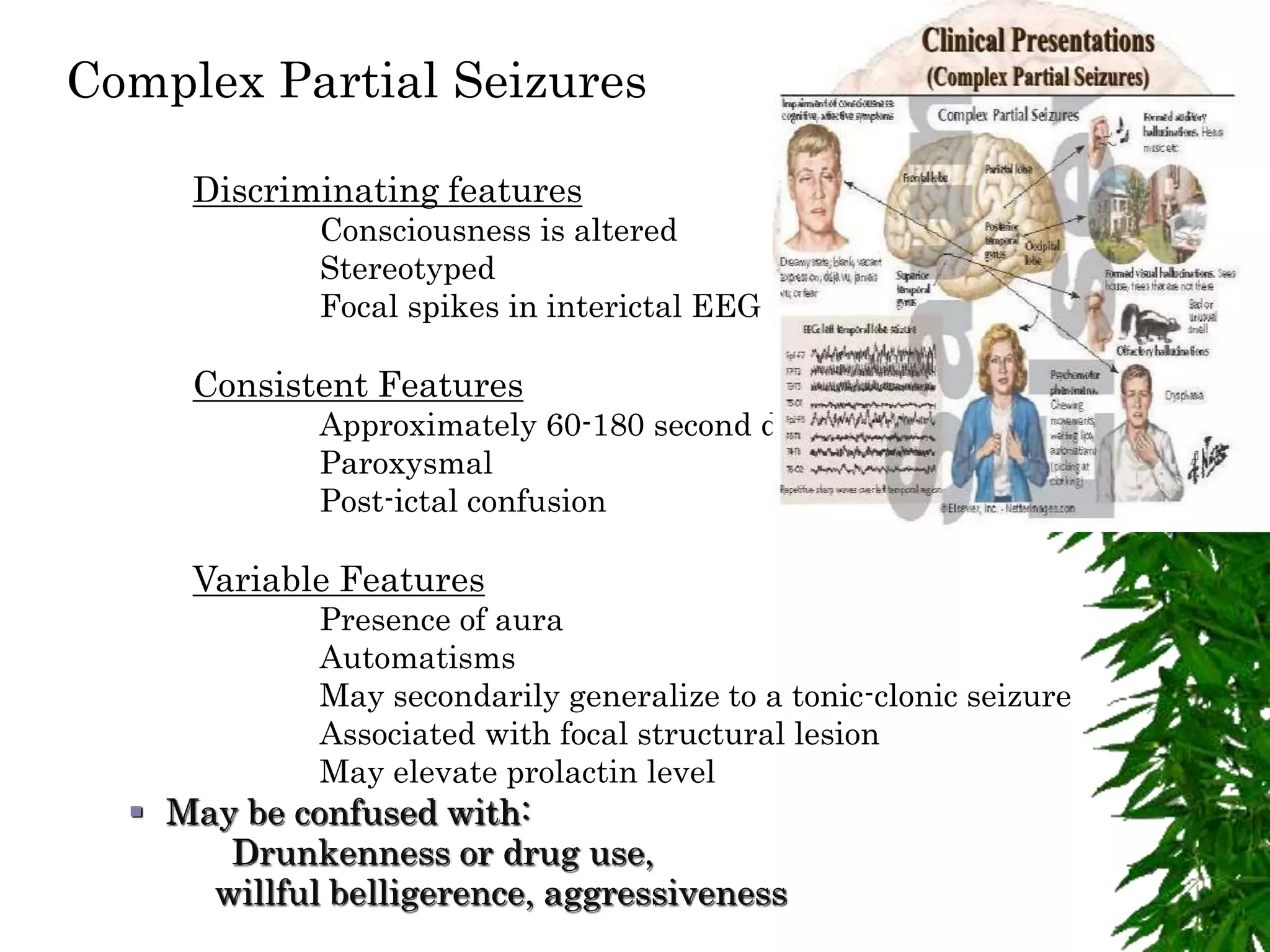
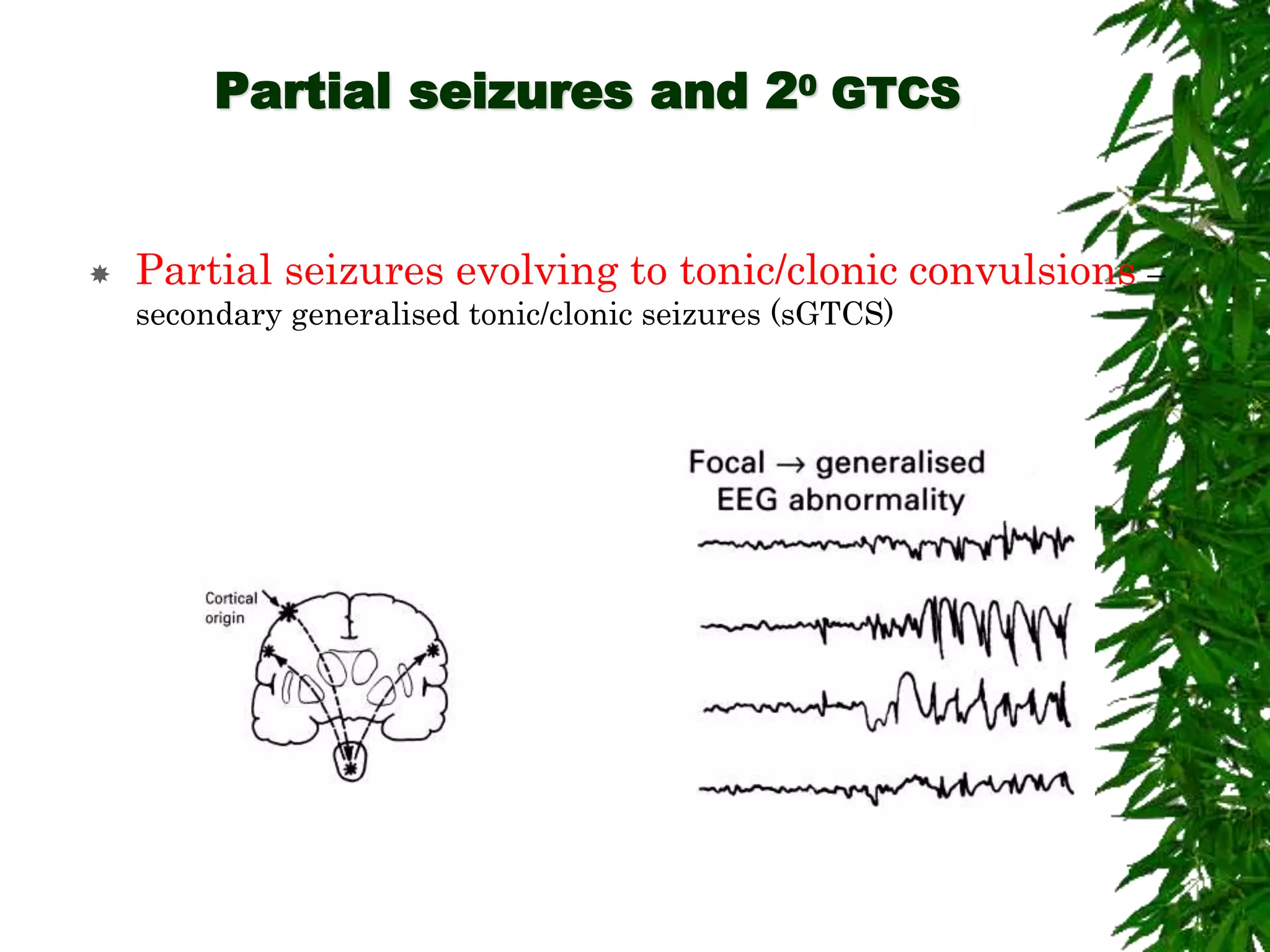
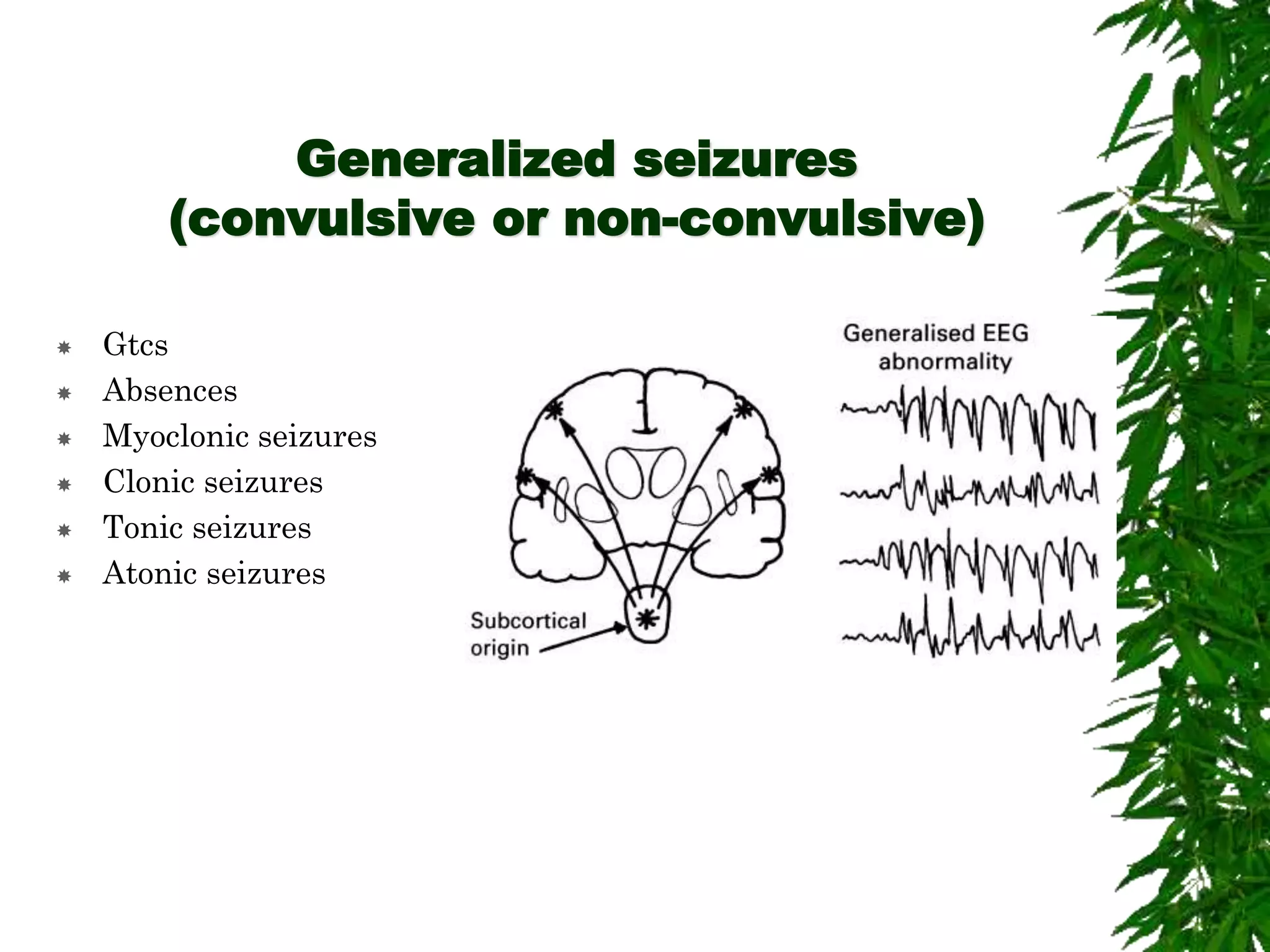
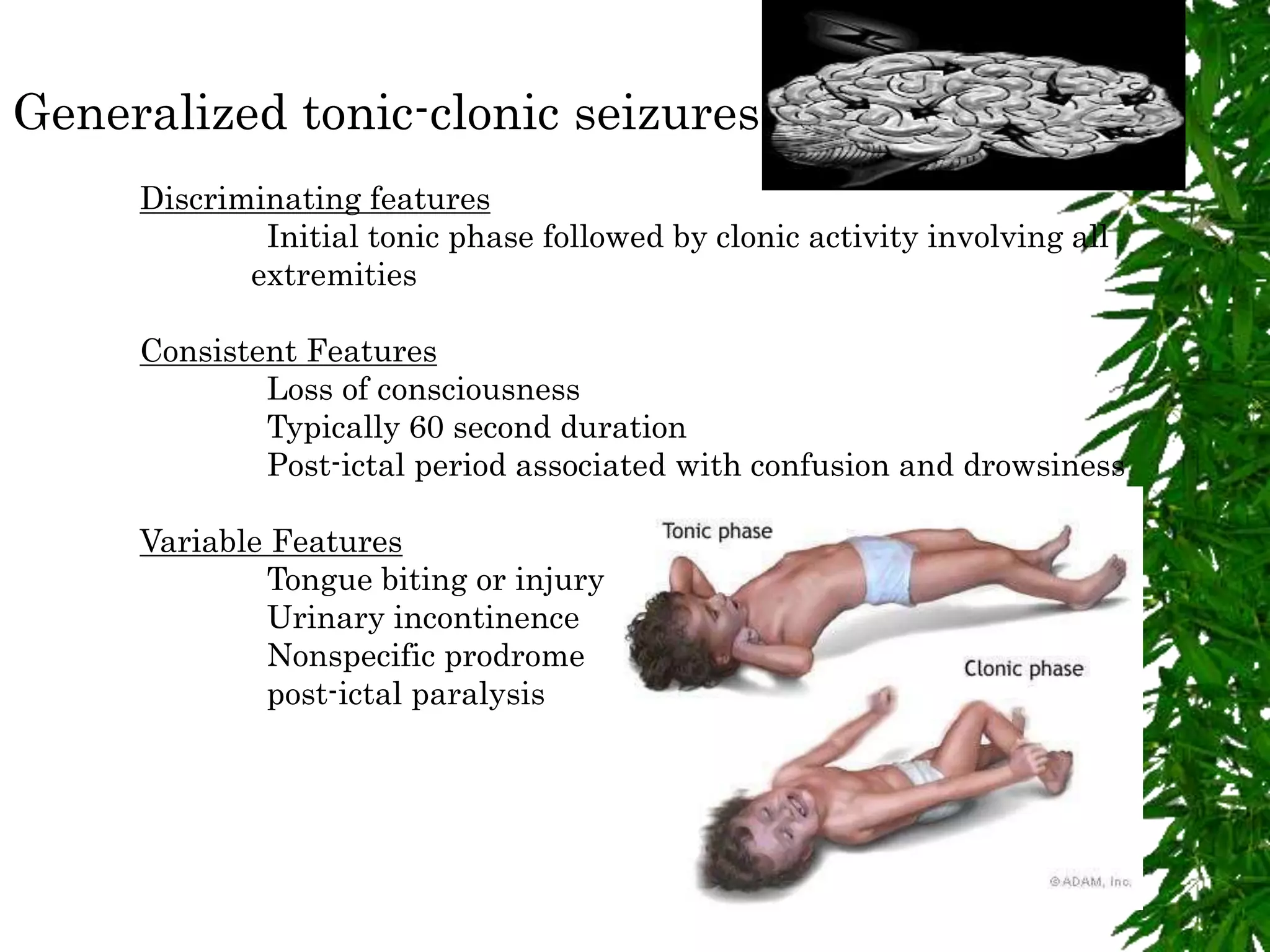
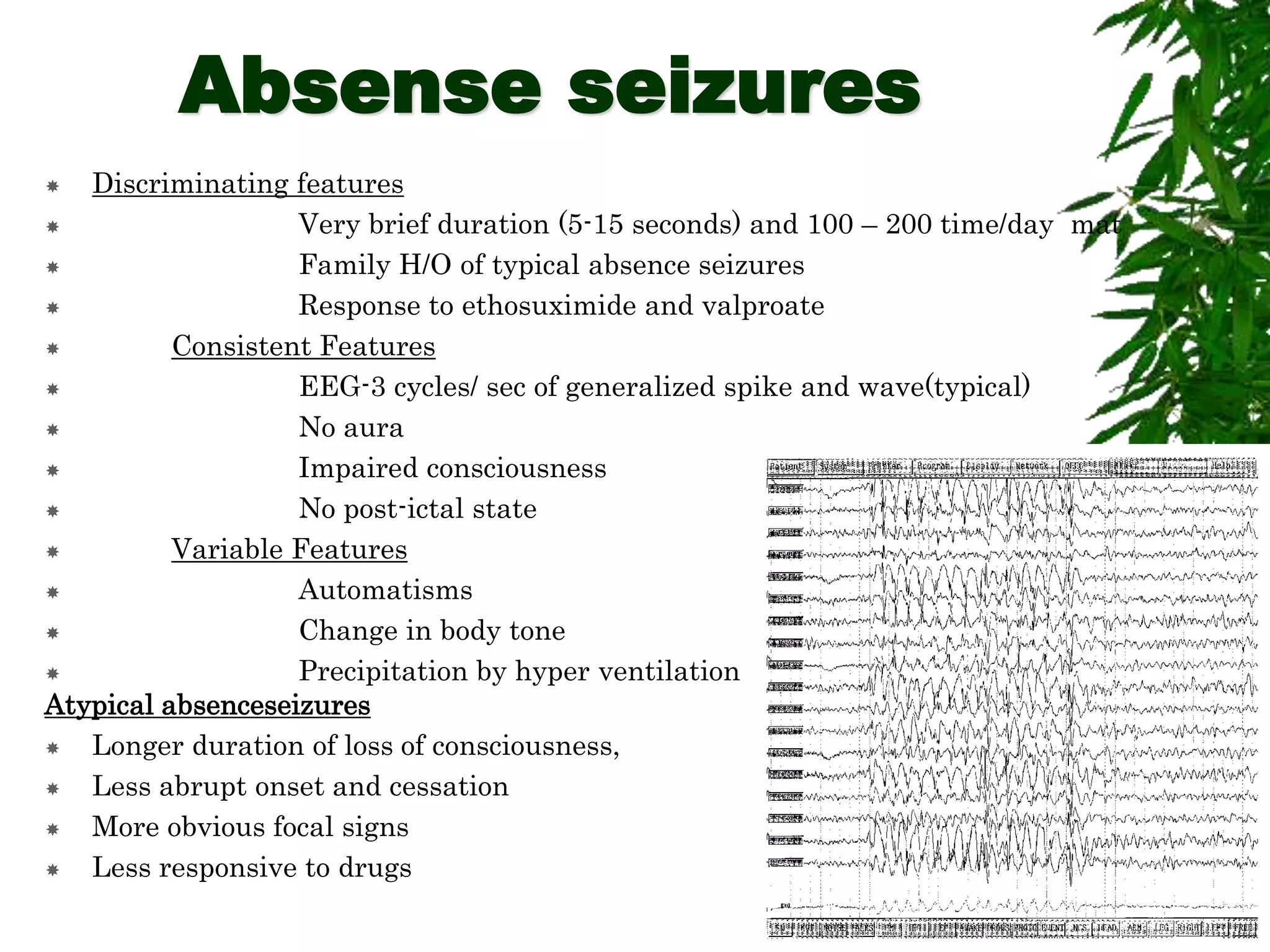
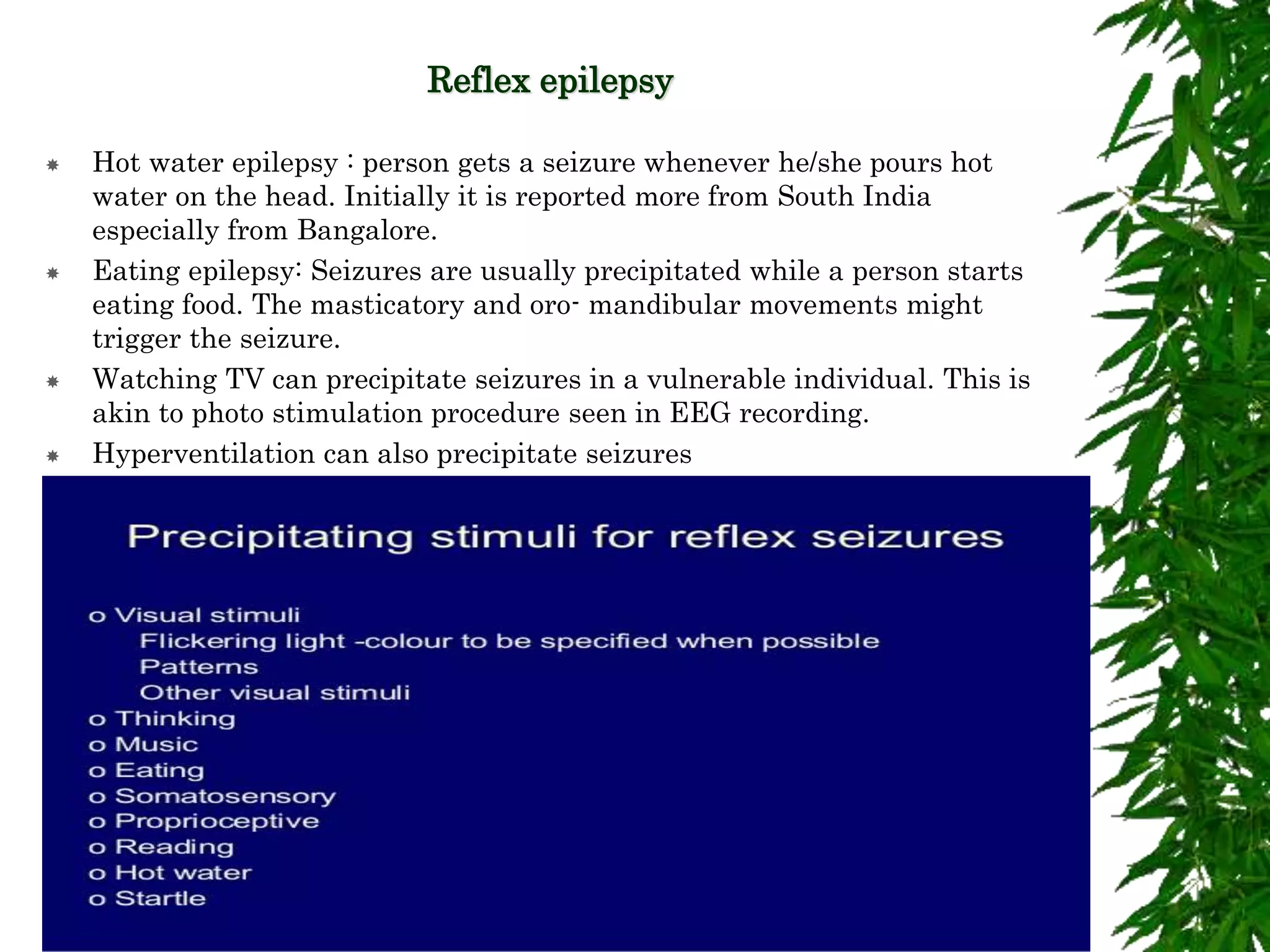
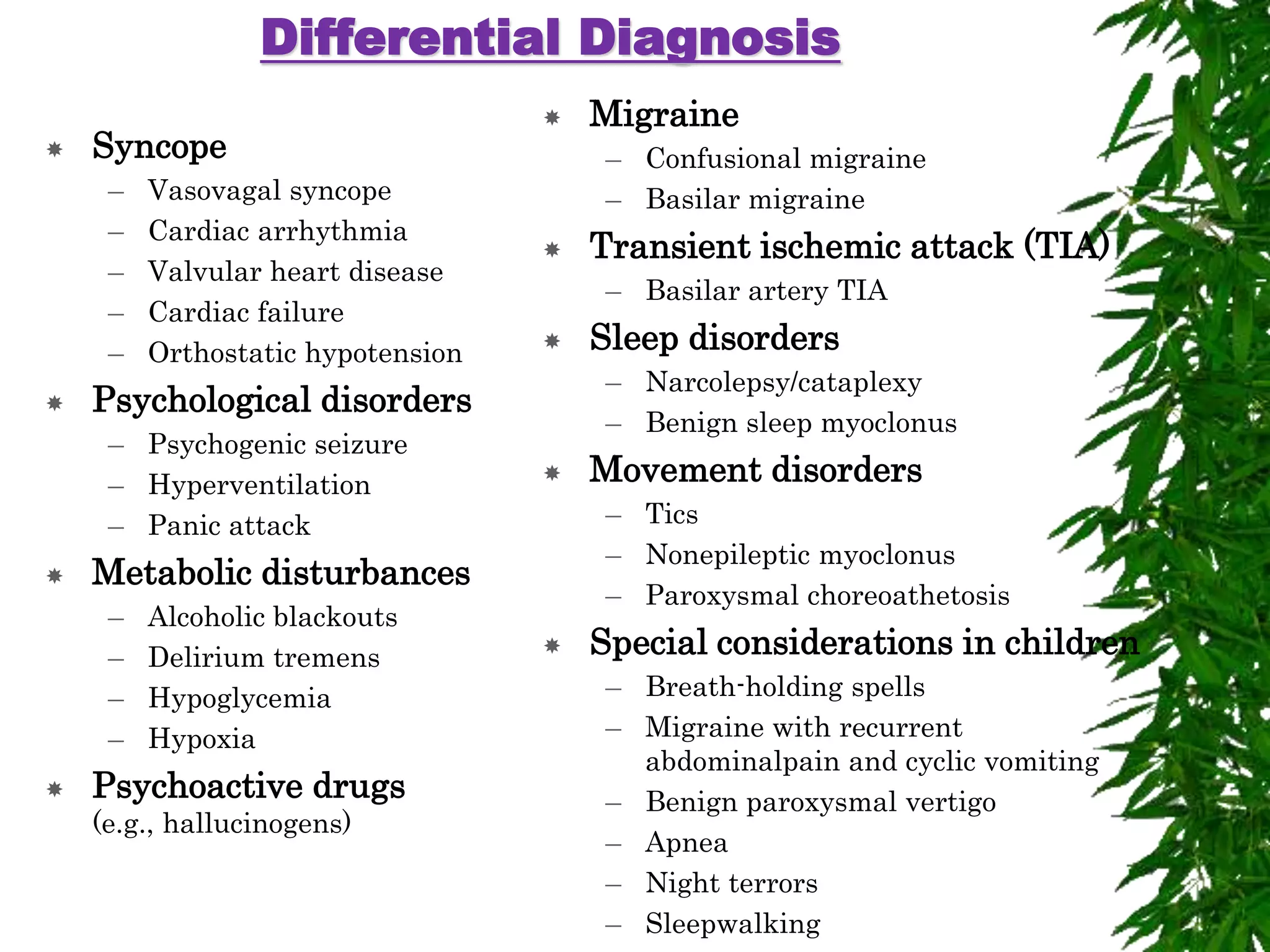
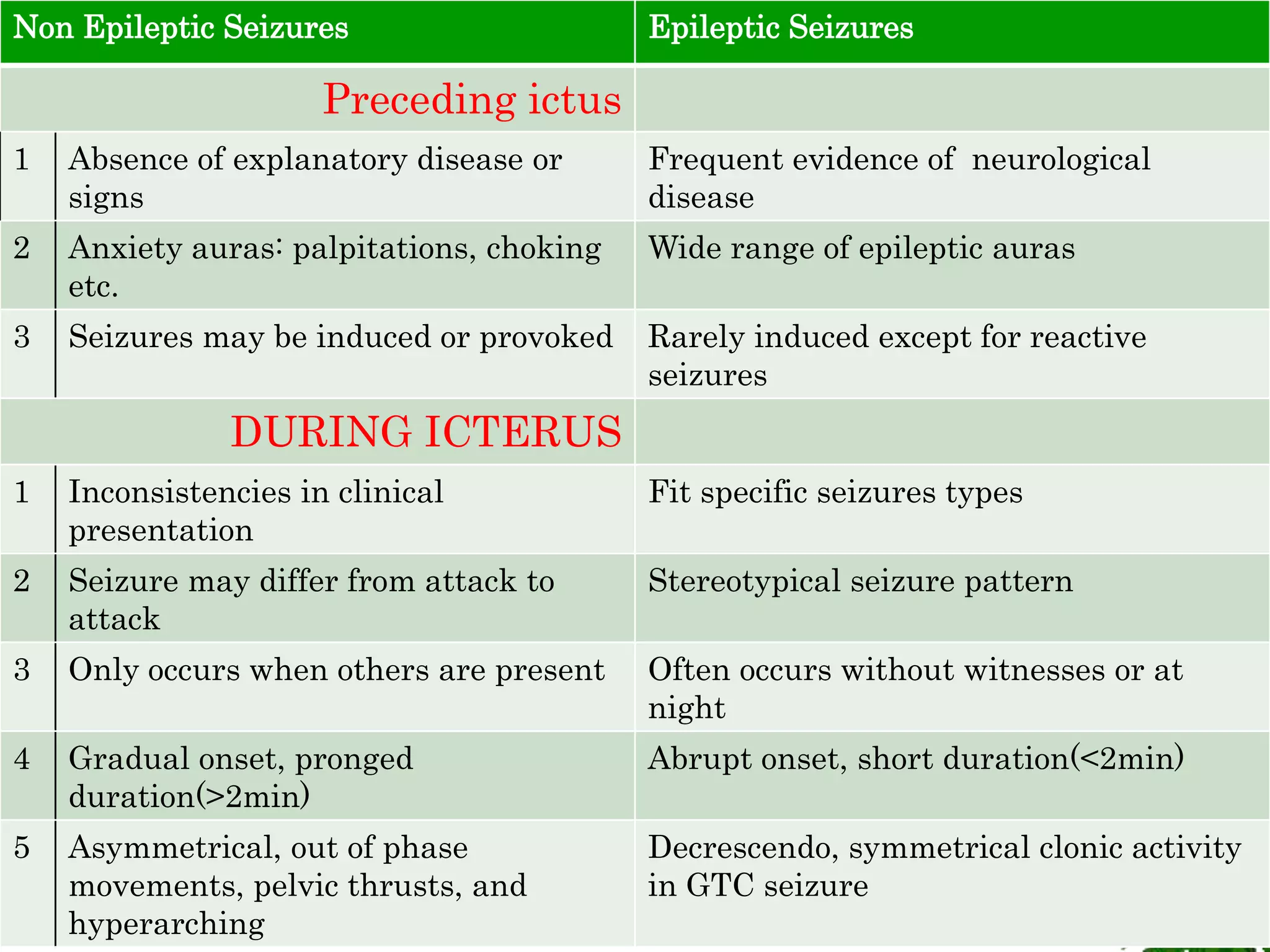
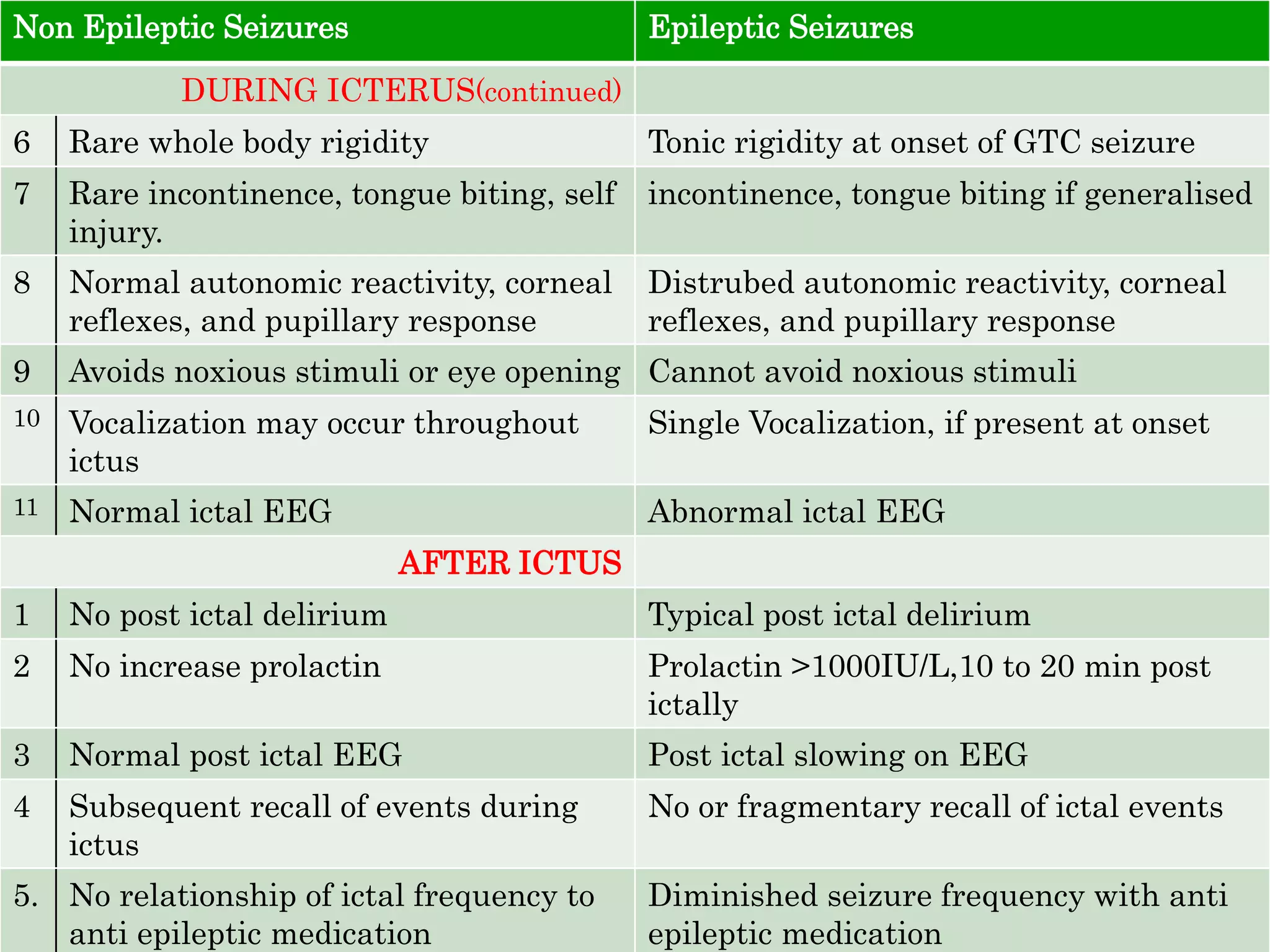
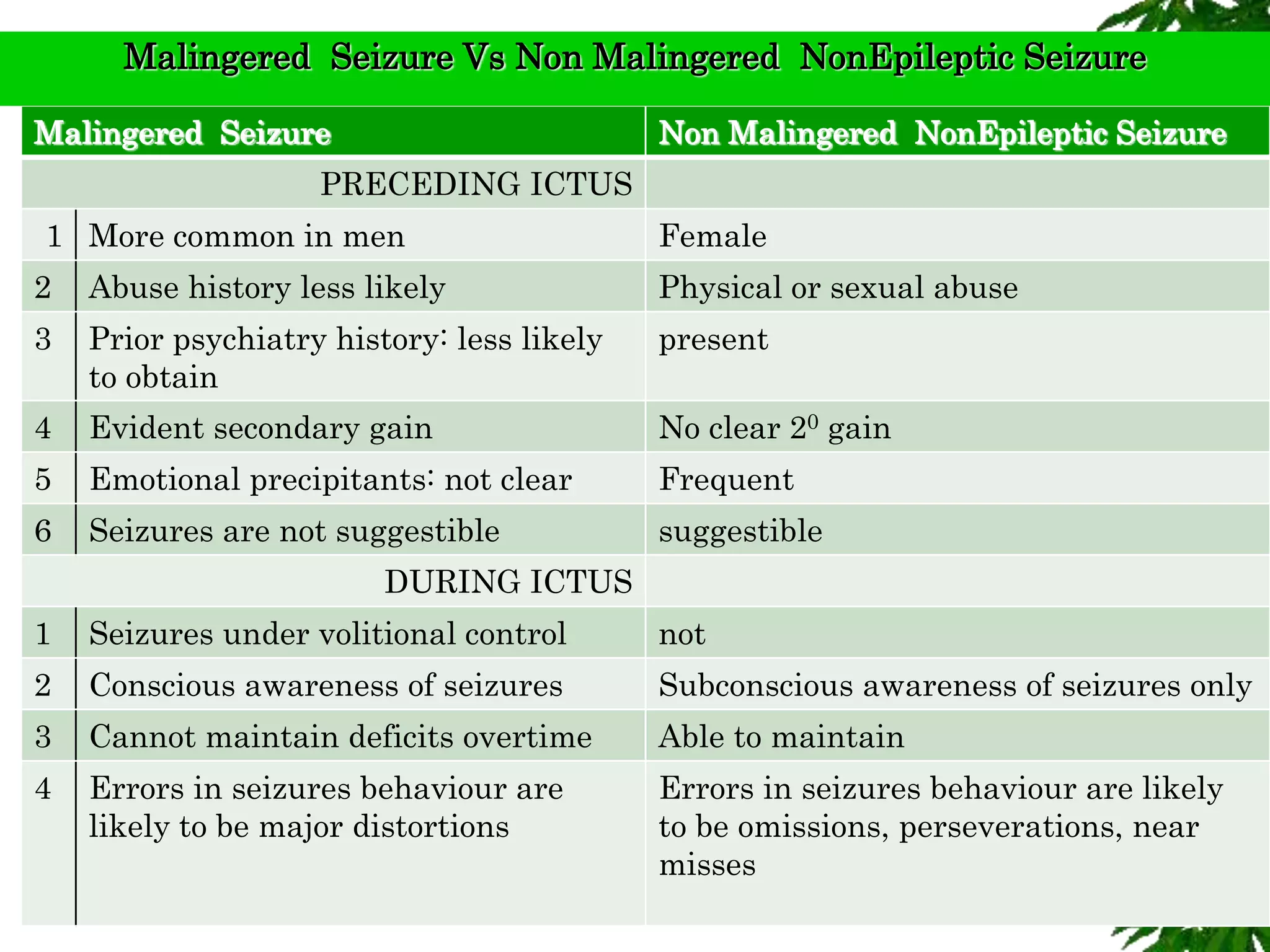
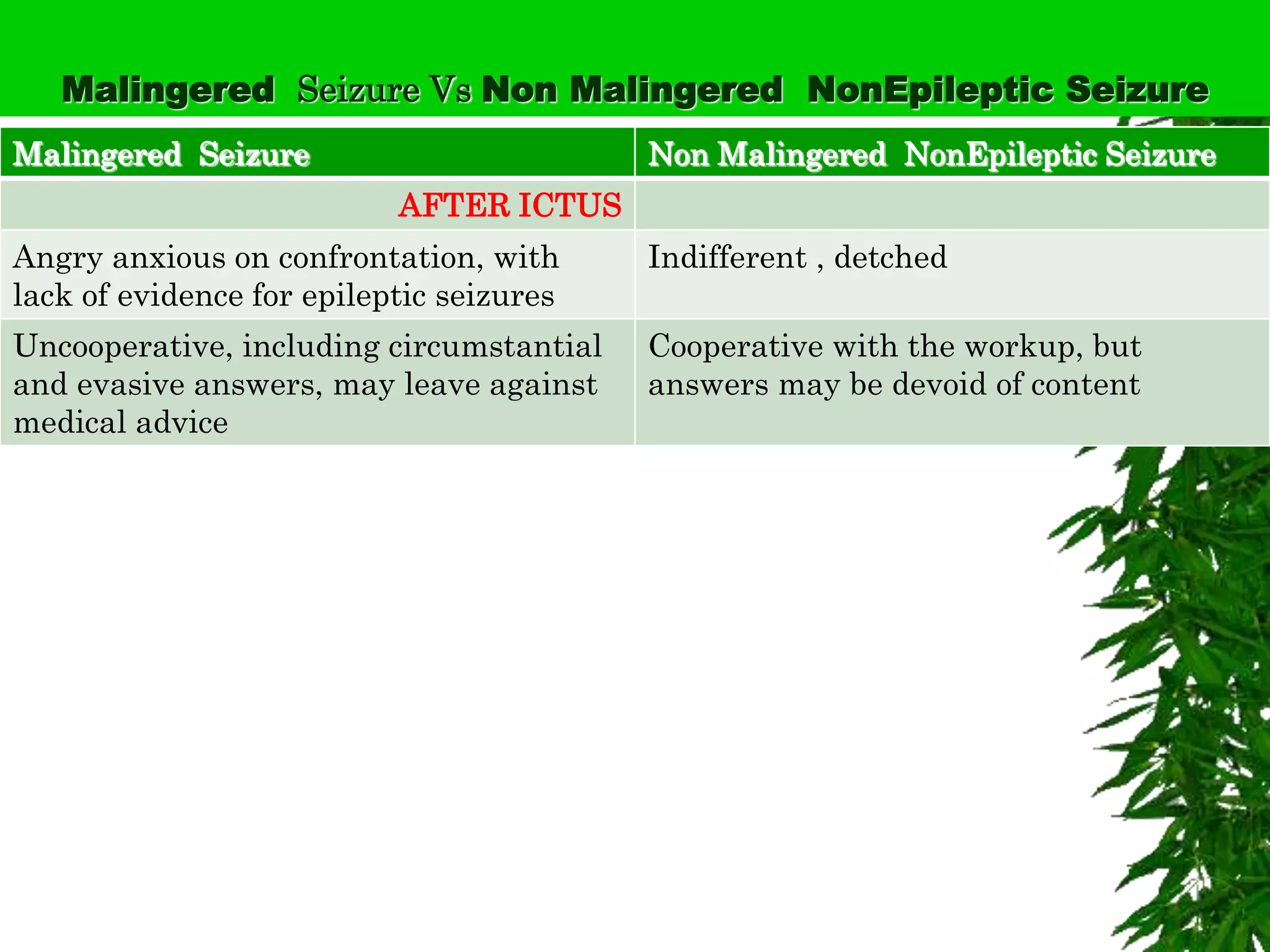
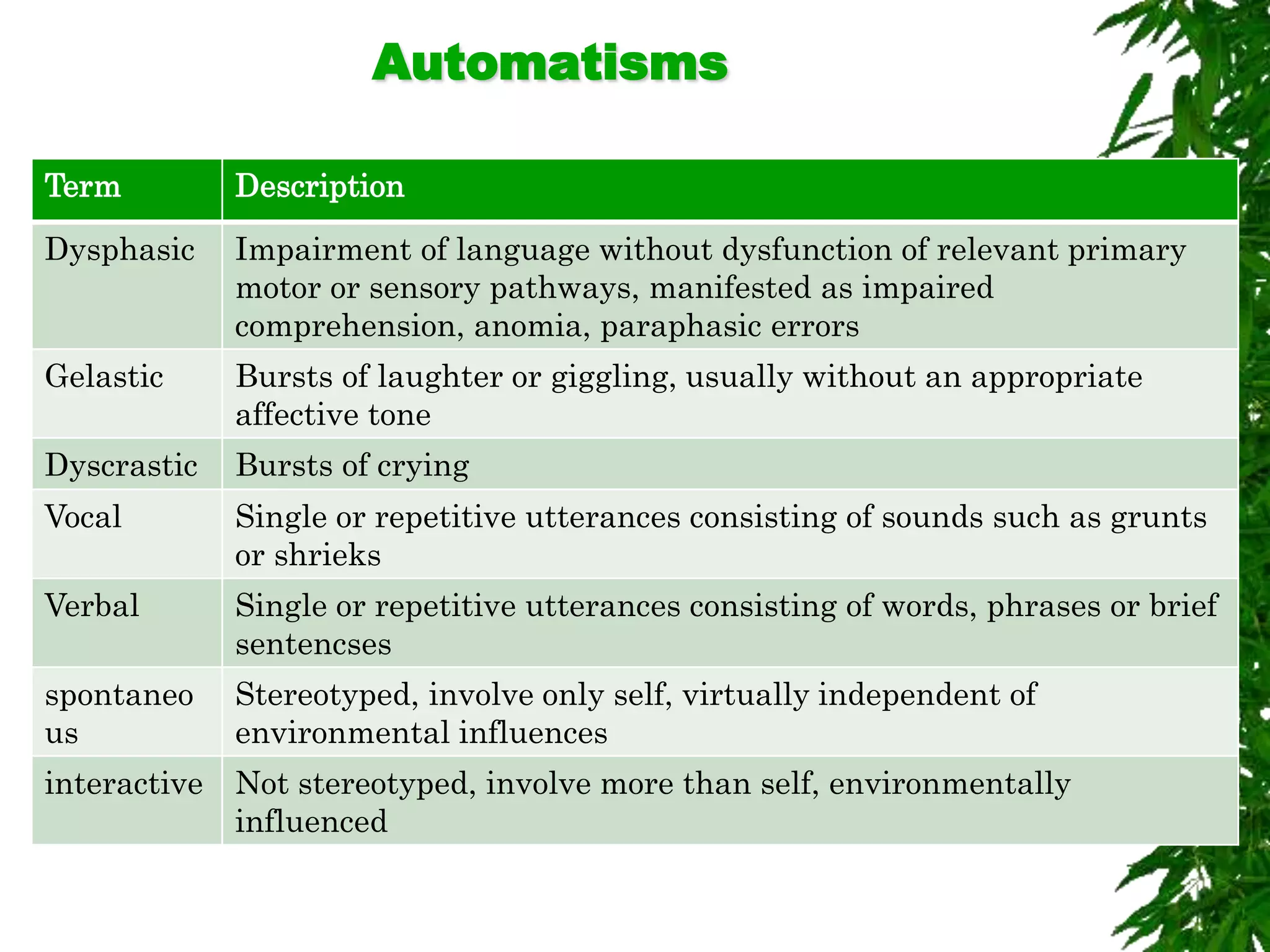
The document discusses neuropsychiatric aspects of epilepsy. It begins with definitions of key terms like seizure, epilepsy, and convulsion. It then provides epidemiological data on epilepsy prevalence and incidence globally. It describes different types of seizures including primary generalized seizures, partial seizures, and epilepsy syndromes. Causes of epilepsy including genetic, acquired, congenital, and withdrawal factors are outlined. Risk factors for developing epilepsy and common seizure triggers are mentioned. The pathophysiology involving glutamate and GABA neurotransmitters is explained. Finally, clinical presentations of different seizure types and differential diagnosis considerations are covered.