Downloaded 71 times


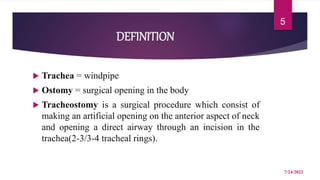
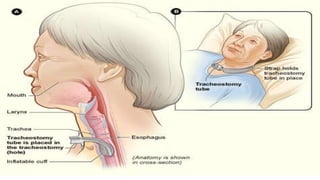
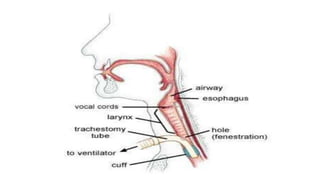


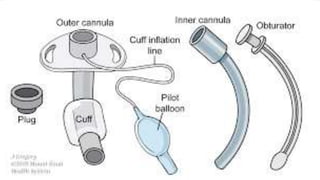
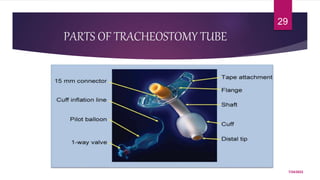
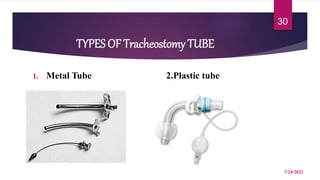
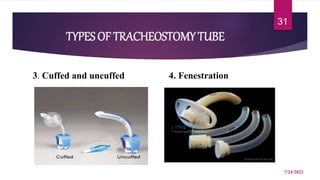



A tracheostomy is a surgical opening made in the neck into the trachea to allow direct access to the breathing tube. It is done to relieve upper airway obstruction, facilitate mechanical ventilation, or remove secretions. Key aspects of tracheostomy care include cleaning and suctioning the tube regularly to keep the airway clear, checking for complications like infection or bleeding, and maintaining proper tube placement and function. Daily care involves monitoring the patient's breathing status and suctioning as needed to prevent obstruction and promote comfort.























































































