Downloaded 91 times





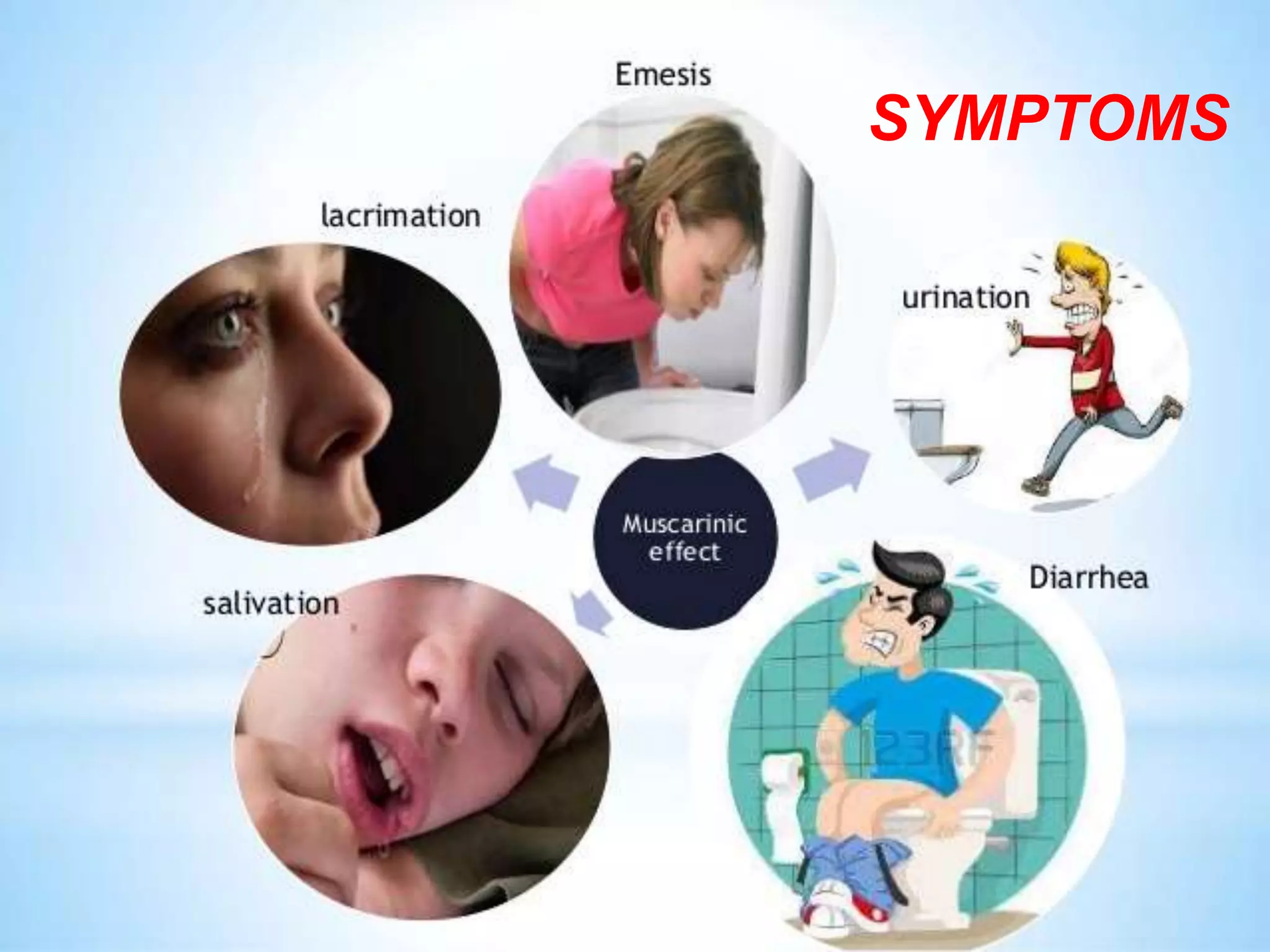




















Organophosphate poisoning is caused by exposure to organophosphates, leading to symptoms such as excessive salivation, muscle tremors, and respiratory failure. Treatment involves airway management, atropine administration, and supportive care, while prevention includes protective gear and immediate washing of exposed skin. Severe cases require monitoring and can involve the use of pralidoxime to reverse poisoning effects.























































































