Download as PDF, PPTX











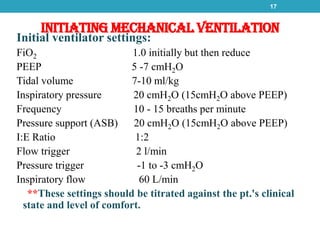





































This document provides information on the care of patients on ventilators and weaning. It begins with definitions of ventilator terminology and then describes the types of ventilators, modes of ventilation, indications for ventilation, initial settings, complications and nursing care considerations. Positive pressure ventilators require an artificial airway while negative pressure ventilators do not. Modes include controlled, assist-control, SIMV, pressure support and others. Nurses must carefully monitor patients, ventilator settings and alarms, suction airways as needed and meet other physiological needs.