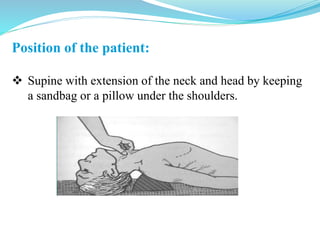
Tracheostomy is a surgical procedure that creates an opening in the trachea to allow for breathing. There are different types including emergency and elective procedures, as well as variations in where the opening is placed. Common indications are for breathing issues from medical conditions like coma, tetanus, or injuries. The procedure involves making an incision in the neck and opening the trachea to insert a tracheostomy tube. Post-operative care requires cleaning and suctioning the tube regularly. Complications can occur immediately during surgery or later from long-term tube use and include bleeding, infection, stenosis, or fistula formation.




























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








