Downloaded 735 times
![References
• http://emedicine.medscape.com/article/149665-overview#a2. Retrieved on the 2nd
March, 2016
• Sampson EL, Candy B, Jones L. Enteral tube feeding for older people with advanced
dementia.Cochrane Database Syst Rev. 2009;(2):CD007209. [PubMed]
• Kimyagarov S, Turgeman D, Fleissig Y, Klid R, Kopel B, Adunsky A. Percutaneous
endoscopic gastrostomy (PEG) tube feeding of nursing home residents is not
associated with improved body composition parameters. J Nutr Health
Aging. 2013;17:162–165. [PubMed]](https://image.slidesharecdn.com/gastrostomy-160311100952/85/Gastrostomy-15-320.jpg)


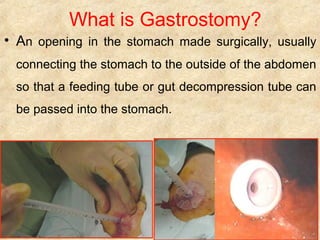
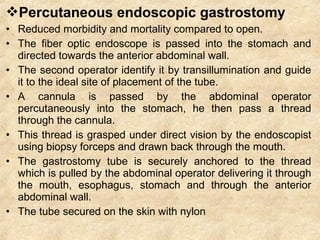
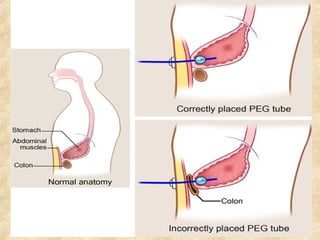
Gastrostomy is a surgical opening made in the stomach to allow for placement of a feeding tube. It is indicated for patients who require prolonged tube feeding for over 4 weeks due to conditions such as neurological swallowing disorders, esophageal cancer, or gastric outlet obstruction. There are two main types - open gastrostomy involving surgical incision and percutaneous endoscopic gastrostomy (PEG) which is performed endoscopically. Complications can include infection, hemorrhage, leakage or displacement of the tube. Gastrostomy allows for safe enteral feeding in patients with poor oral intake who have a functional gastrointestinal system.










































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)












