Downloaded 556 times

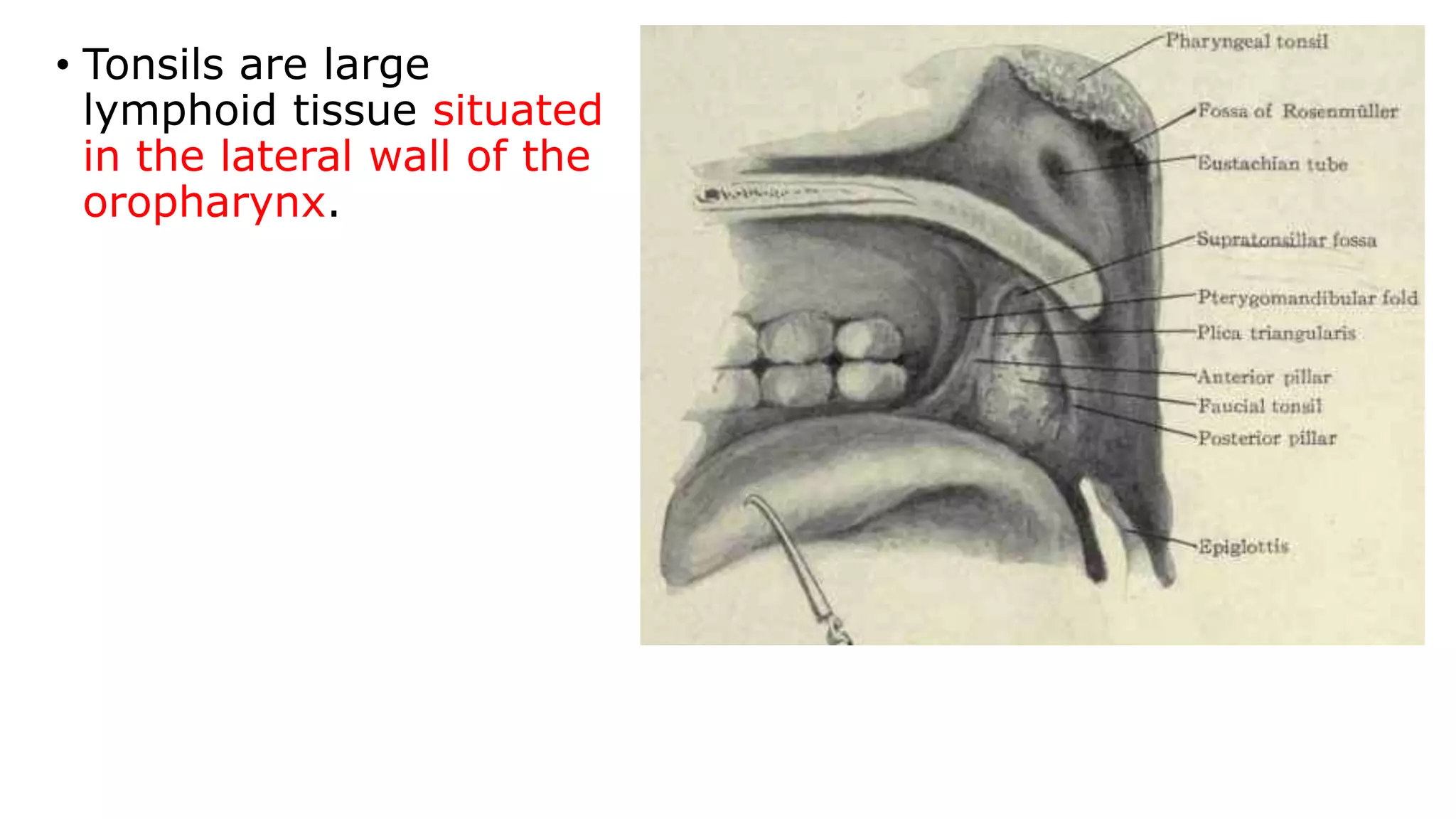







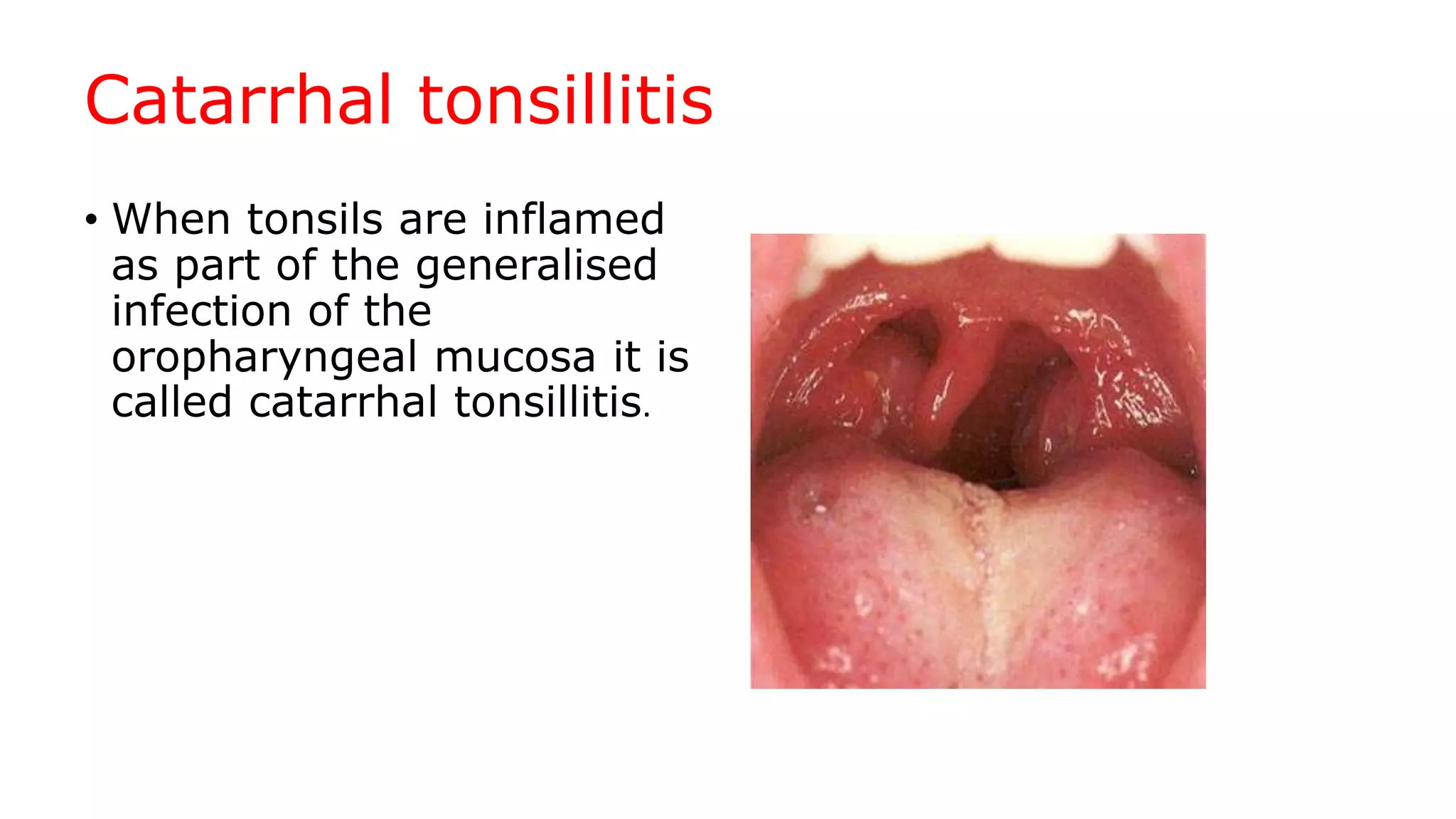












Tonsillitis is an infection of the tonsils, which are lymphoid tissue located in the throat. It can be acute or chronic. Common causes include viral or bacterial infections. Symptoms include pain and difficulty swallowing. Complications may include peritonsillar abscesses or spread of infection. Treatment involves rest, fluids, pain medications, and antibiotics. Tonsillectomy may be required in cases of recurrent infections or abscesses.






























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












