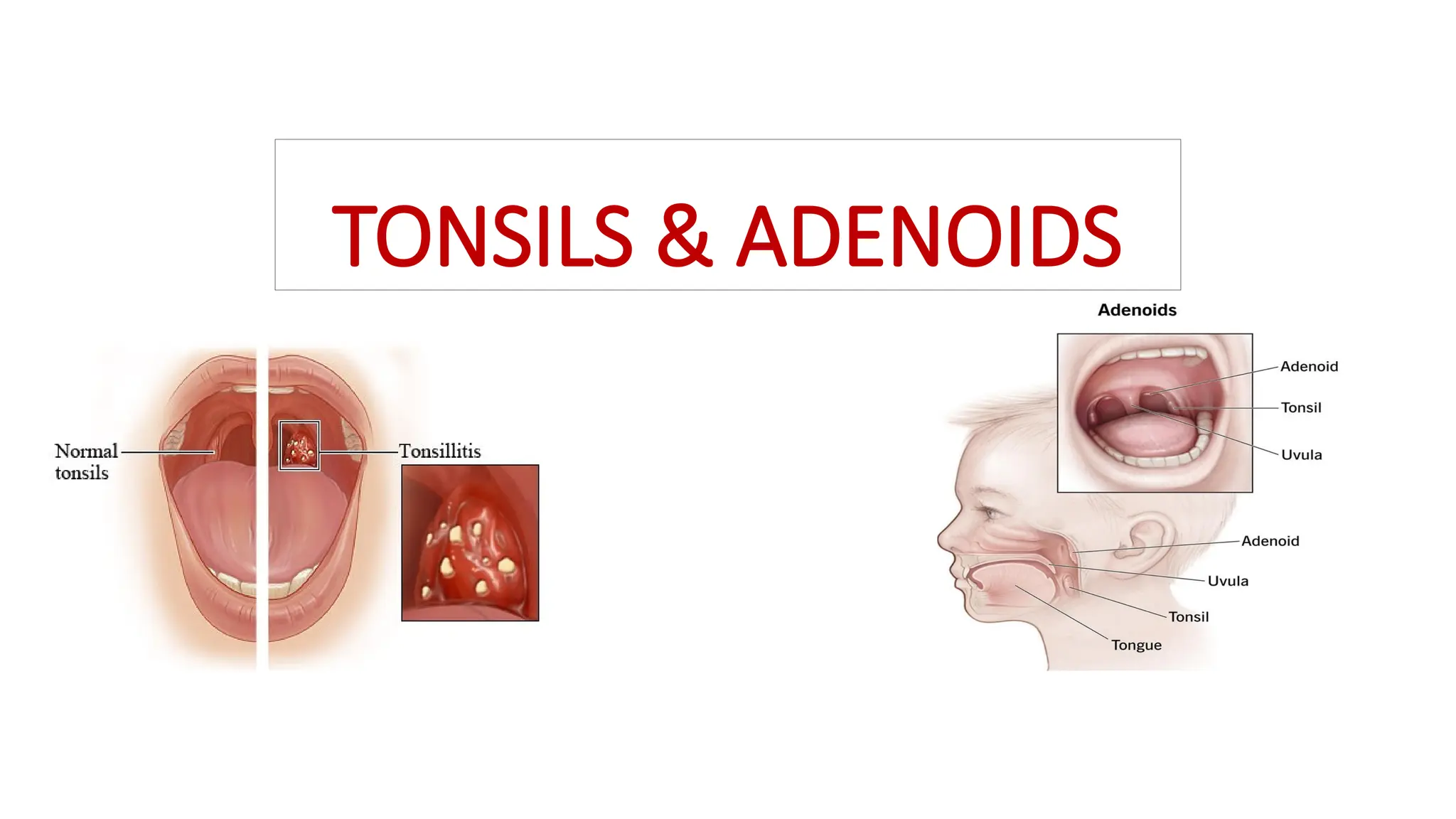
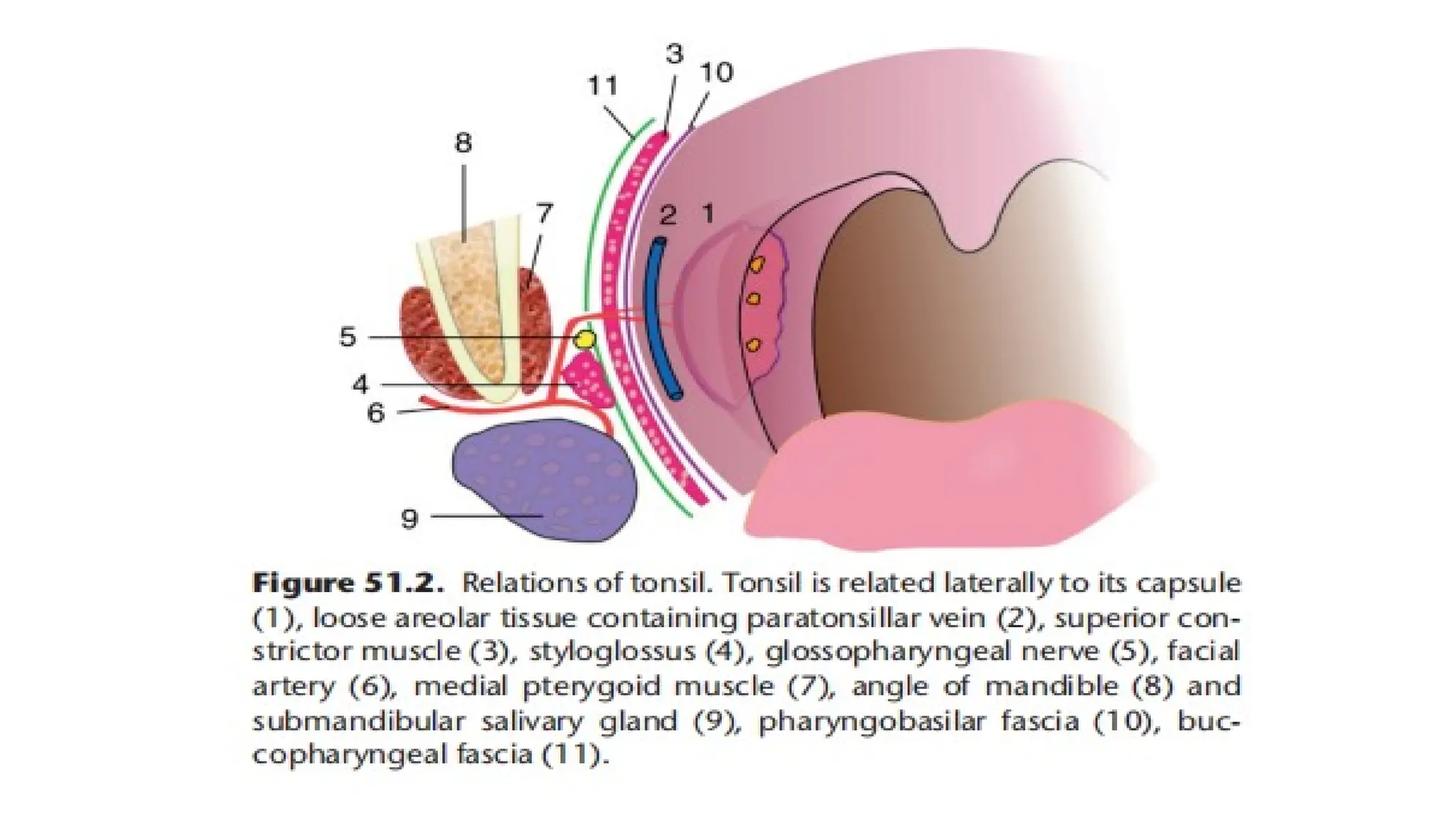
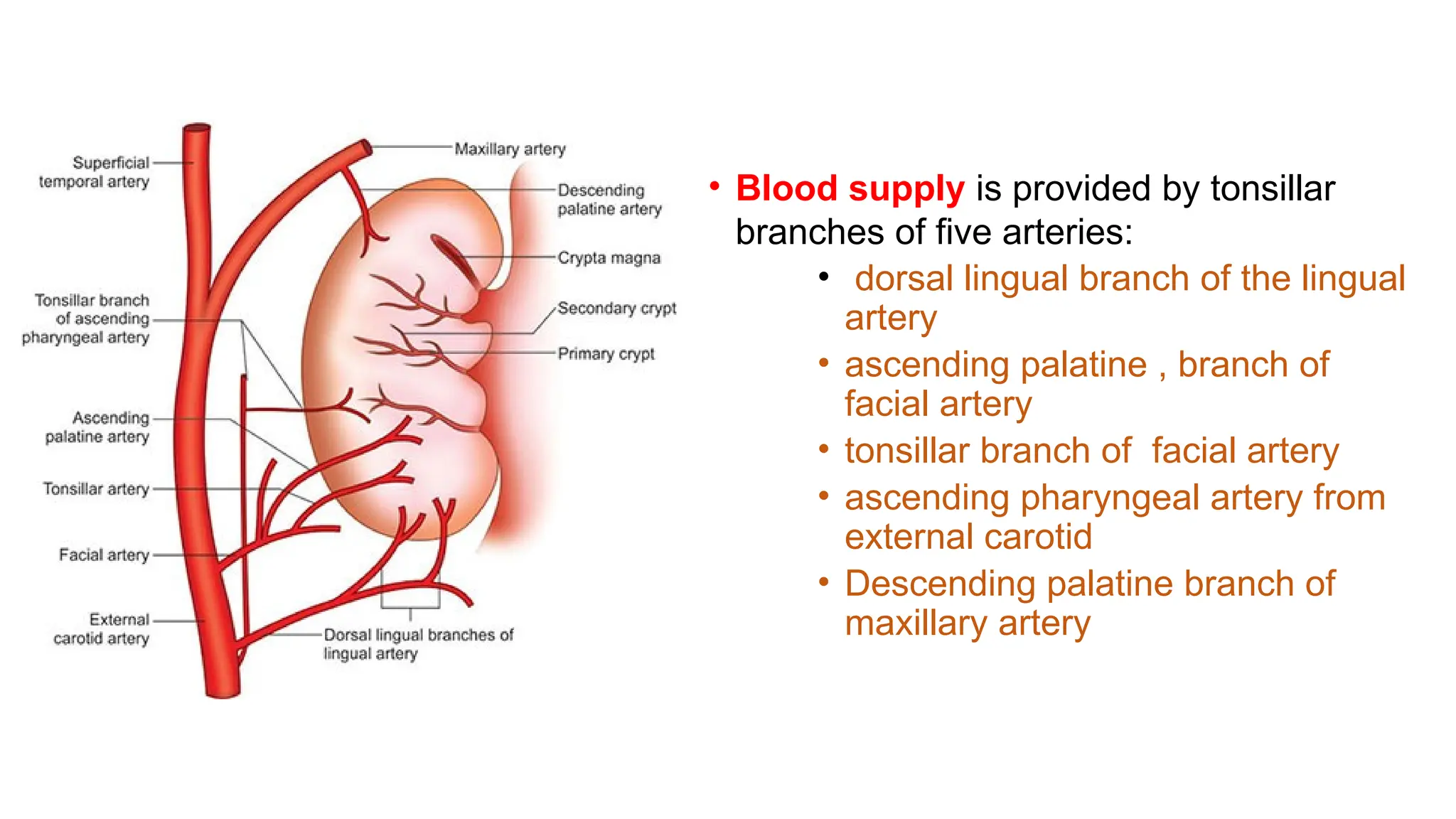
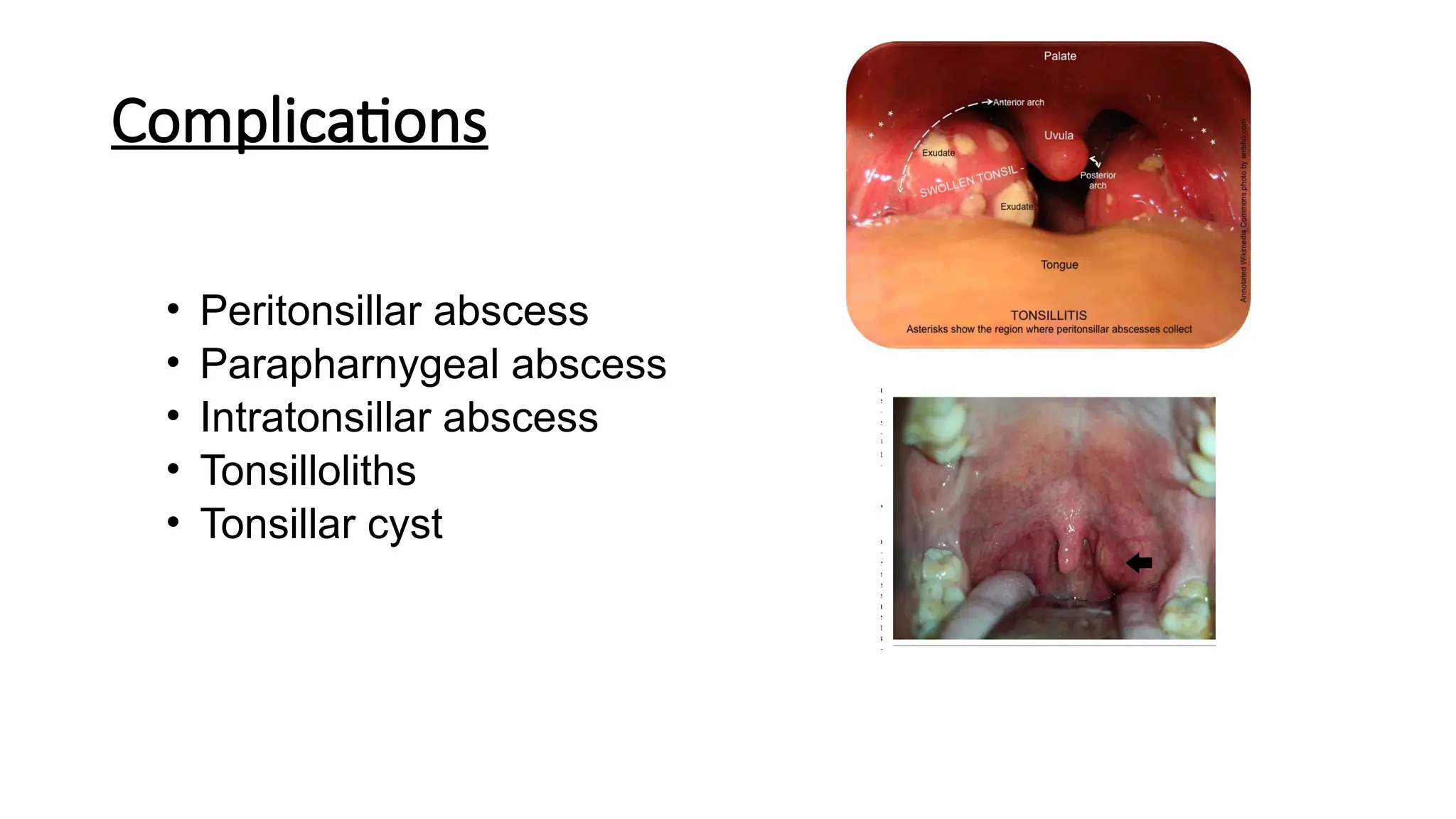
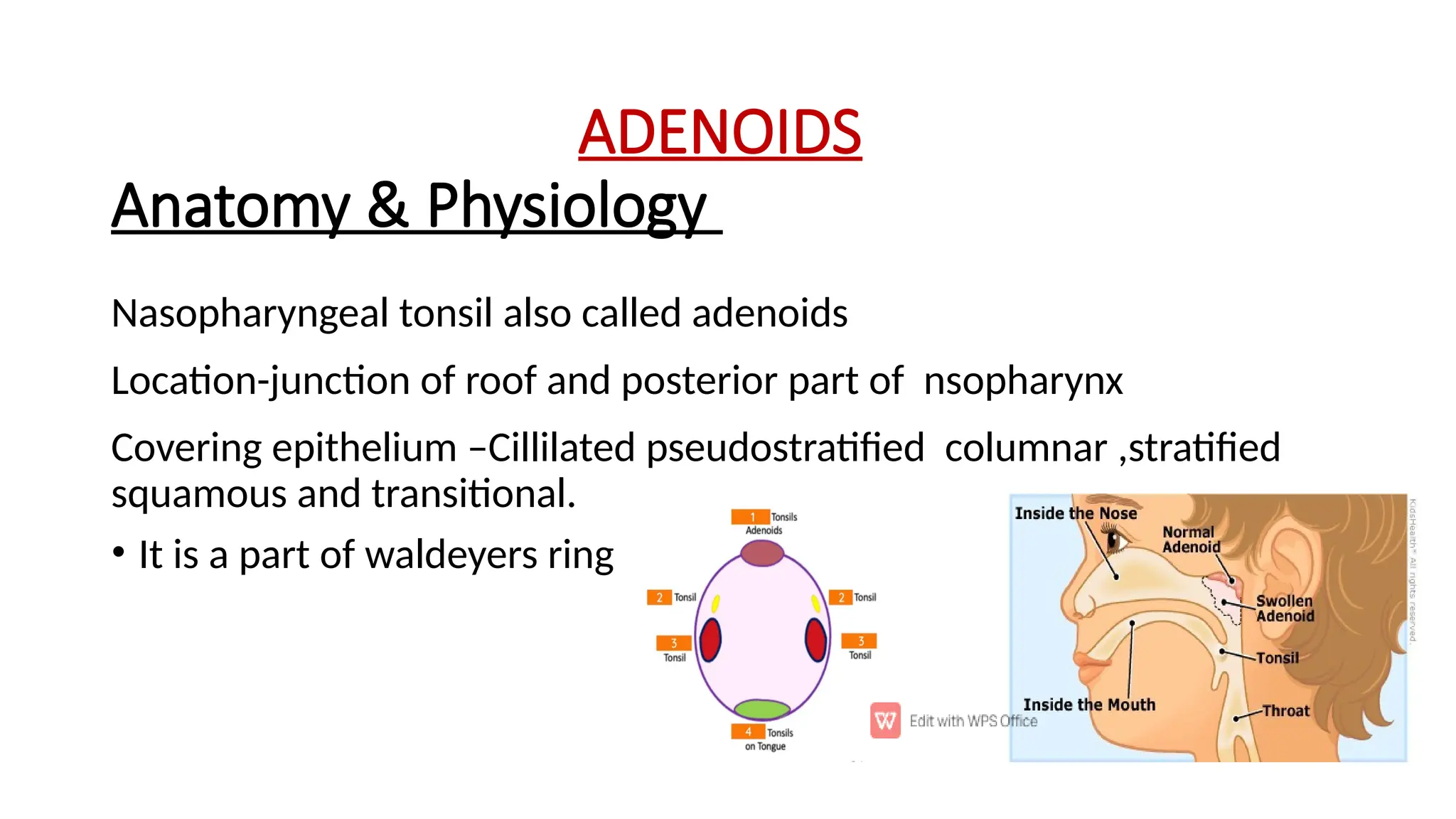
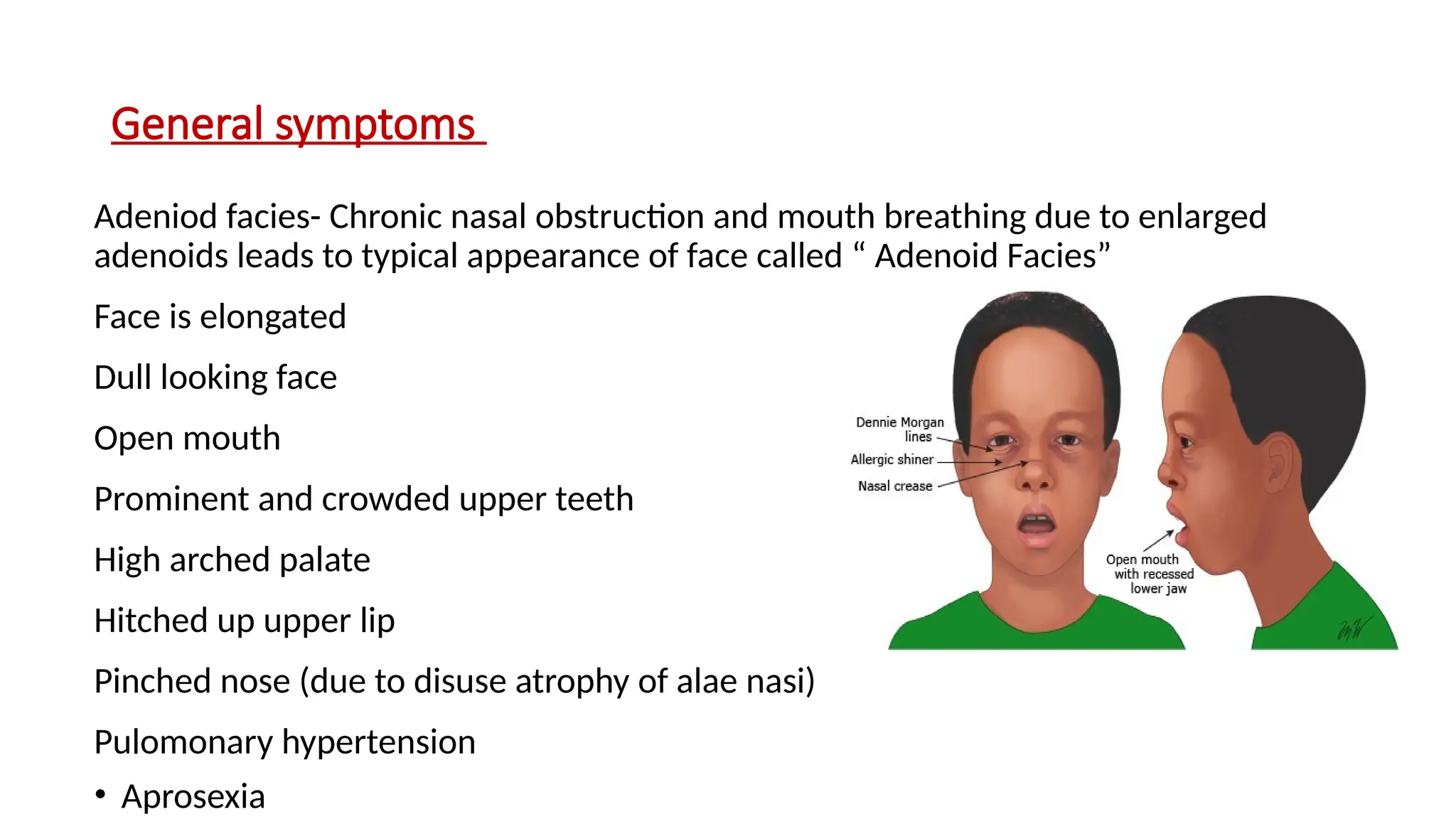
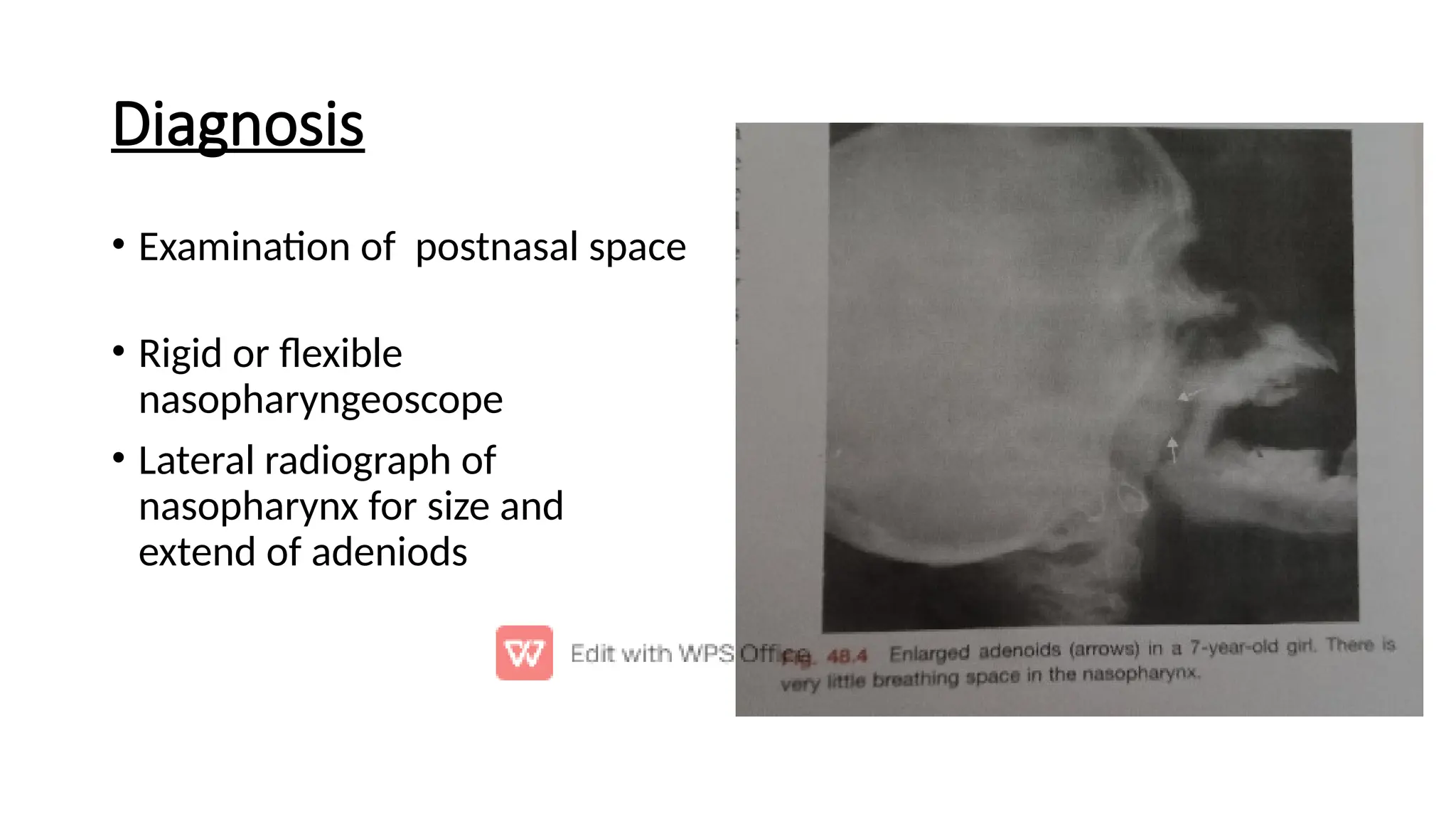
The document provides a detailed overview of tonsils and adenoids, including their anatomy, functions, and treatment of conditions such as tonsillitis and chronic tonsillitis. Tonsils are essential for the immune system and can become inflamed due to infections, leading to various types of tonsillitis, while adenoids, located in the nasopharynx, can cause nasal obstruction and other respiratory issues when enlarged. Treatments vary based on severity and may include medications, procedural interventions like tonsillectomy or adenoidectomy.