Downloaded 100 times






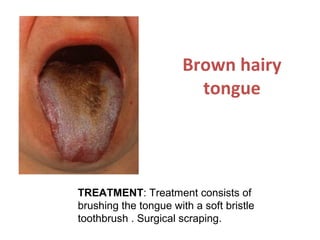

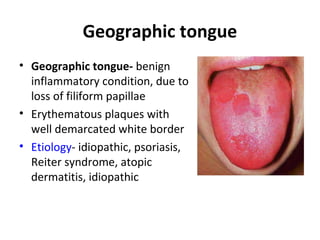



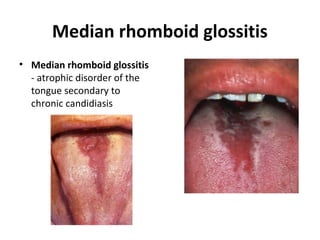
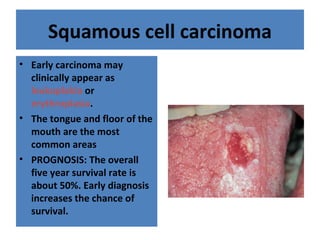
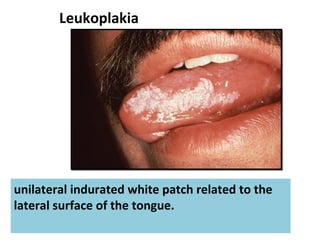


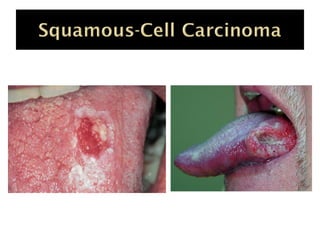
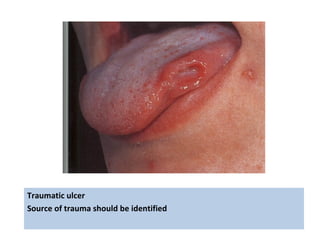


1. The document discusses various diseases and disorders that can affect the tongue, including burning mouth syndrome (glossodynia), glossitis, geographic tongue, hairy tongue, and cancers like squamous cell carcinoma. 2. It describes the clinical examination of the tongue involving inspection, palpation, and function evaluation. Common lesions seen on the tongue are also outlined. 3. Treatment depends on the specific condition but may include antibiotics for infections, tricyclic antidepressants for burning mouth syndrome, improved oral hygiene for hairy tongue, and biopsy or surgery for suspected cancers.




































































































