



![A chelating agent could be given orally, intramuscularly, or
intravenously.
Chelation therapy for acute inorganic mercury poisoning can
be done with DMSA, 2,3-dimercapto-1-propanesulfonic acid
(DMPS), D-penicillamine (DPCN), or dimercaprol (BAL).[1]
Only DMSA is FDA-approved for use in children for treating
mercury poisoning.
correct dosage is required, as inappropriate dosages
increase toxicity.](https://image.slidesharecdn.com/mercuryhazardsandtoxicity-161113205128/85/Mercury-hazards-and-toxicity-17-320.jpg)


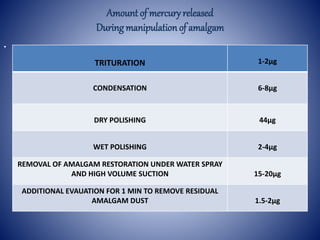
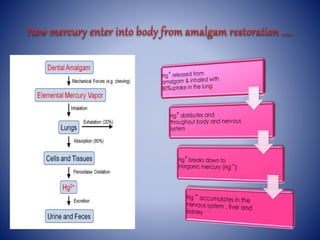
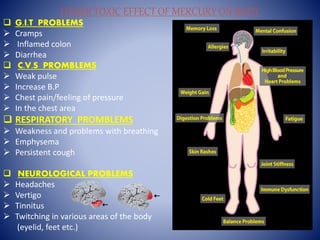
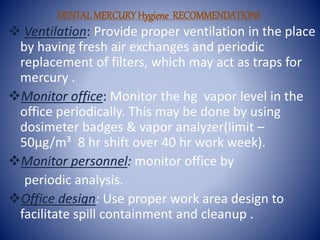
The document discusses the toxicity and hazards of mercury exposure from dental amalgam fillings. It notes that amalgam fillings are 50% mercury and their removal can generate mercury vapors which are inhaled or ingested. It outlines the various ways mercury is released during dental procedures and the toxic effects it can have on the body. The document provides recommendations for dental offices to reduce mercury exposure through improved ventilation, equipment, hygiene practices and waste disposal. It also discusses alternatives to dental amalgam like mercury-free alloys and treatments for mercury toxicity like chelation therapy.































































































