Downloaded 204 times
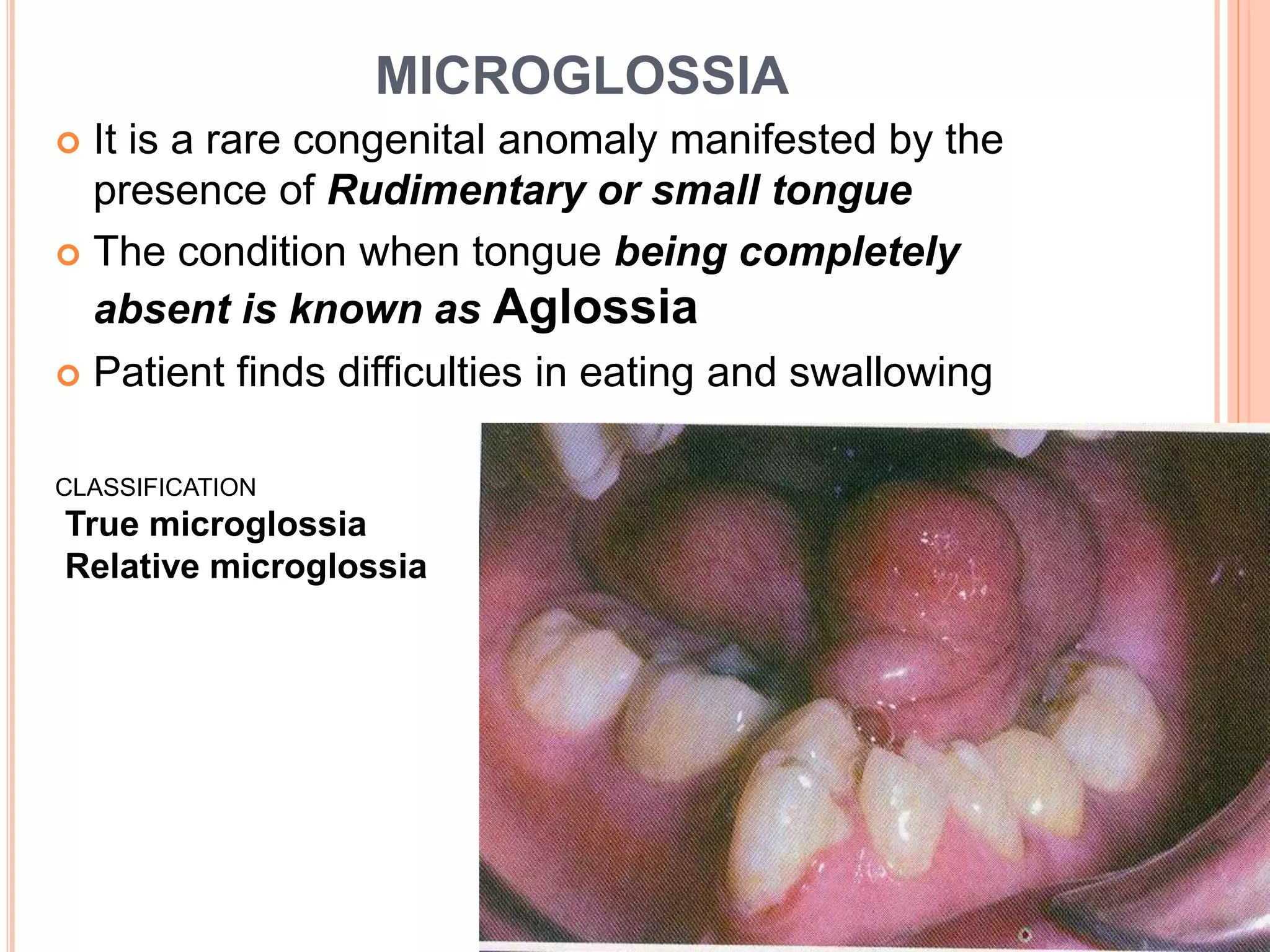
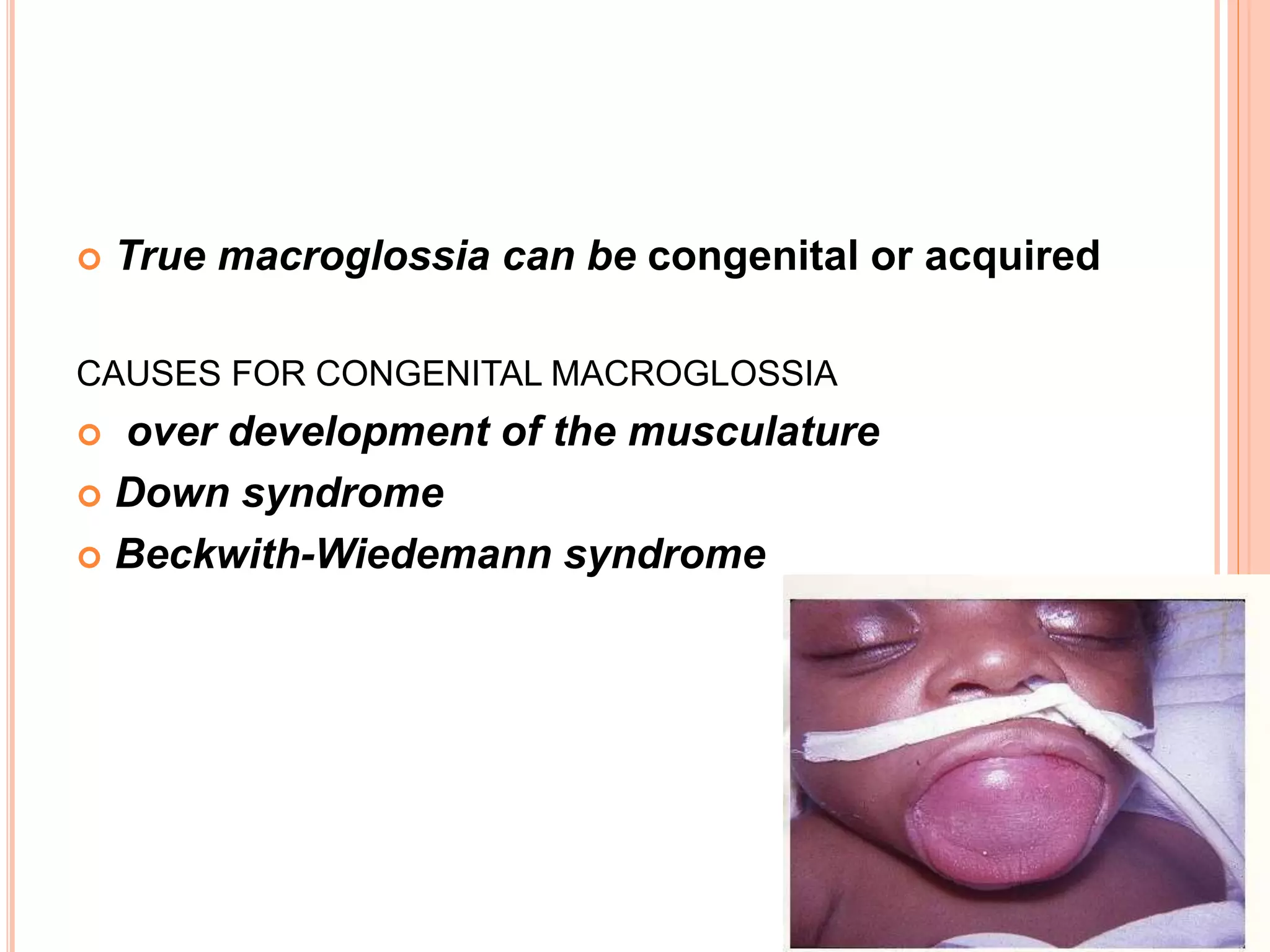

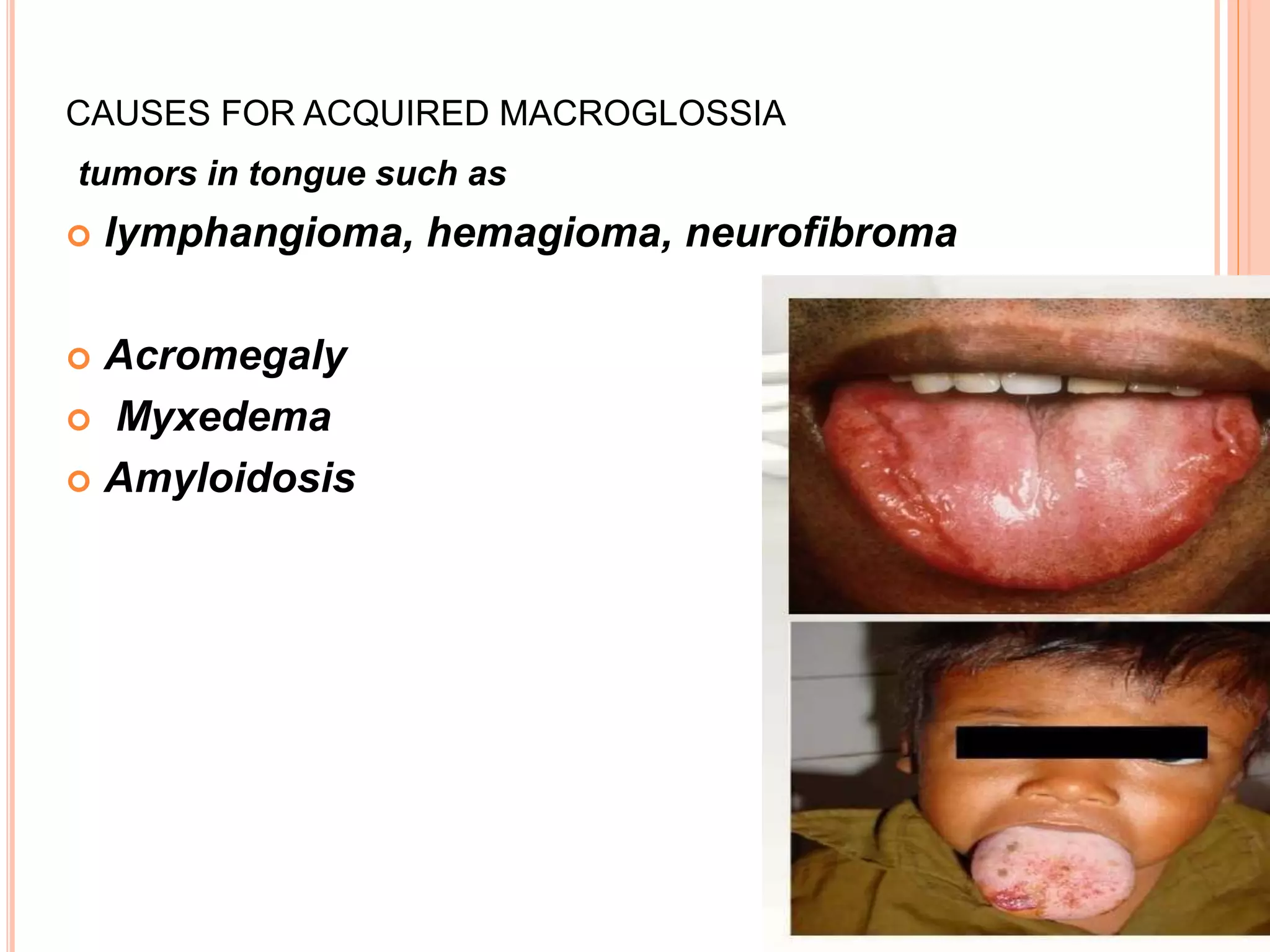

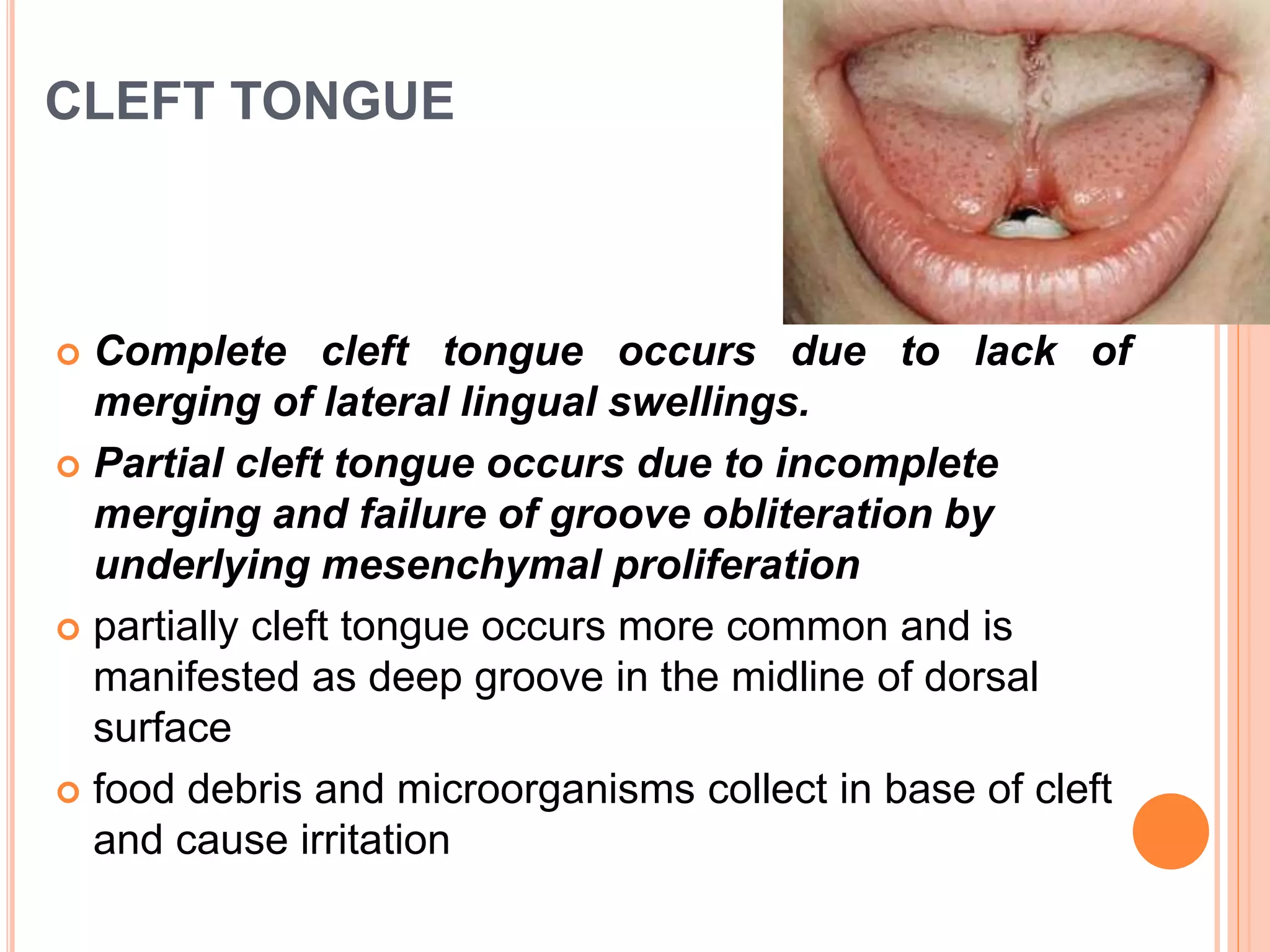
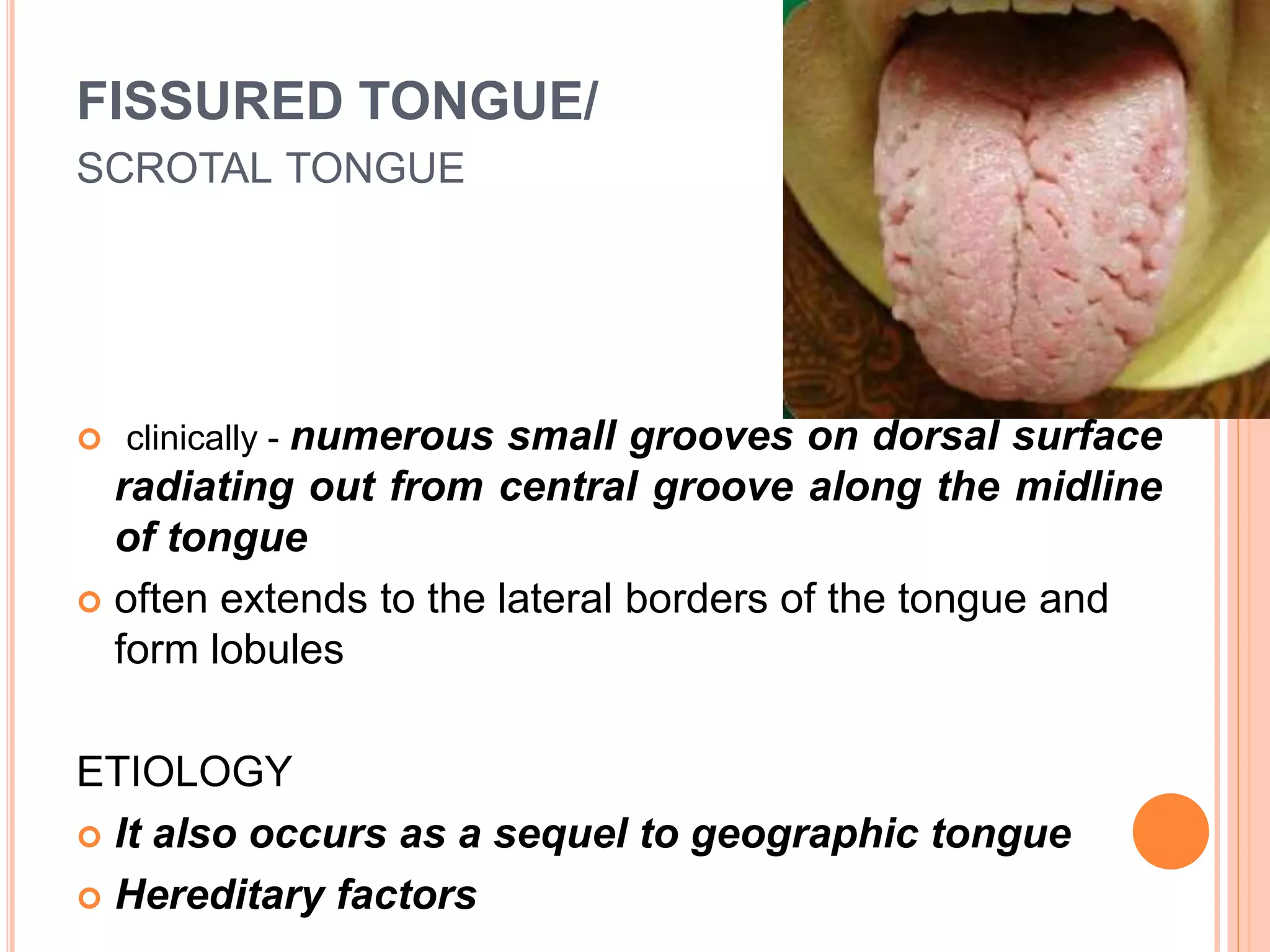
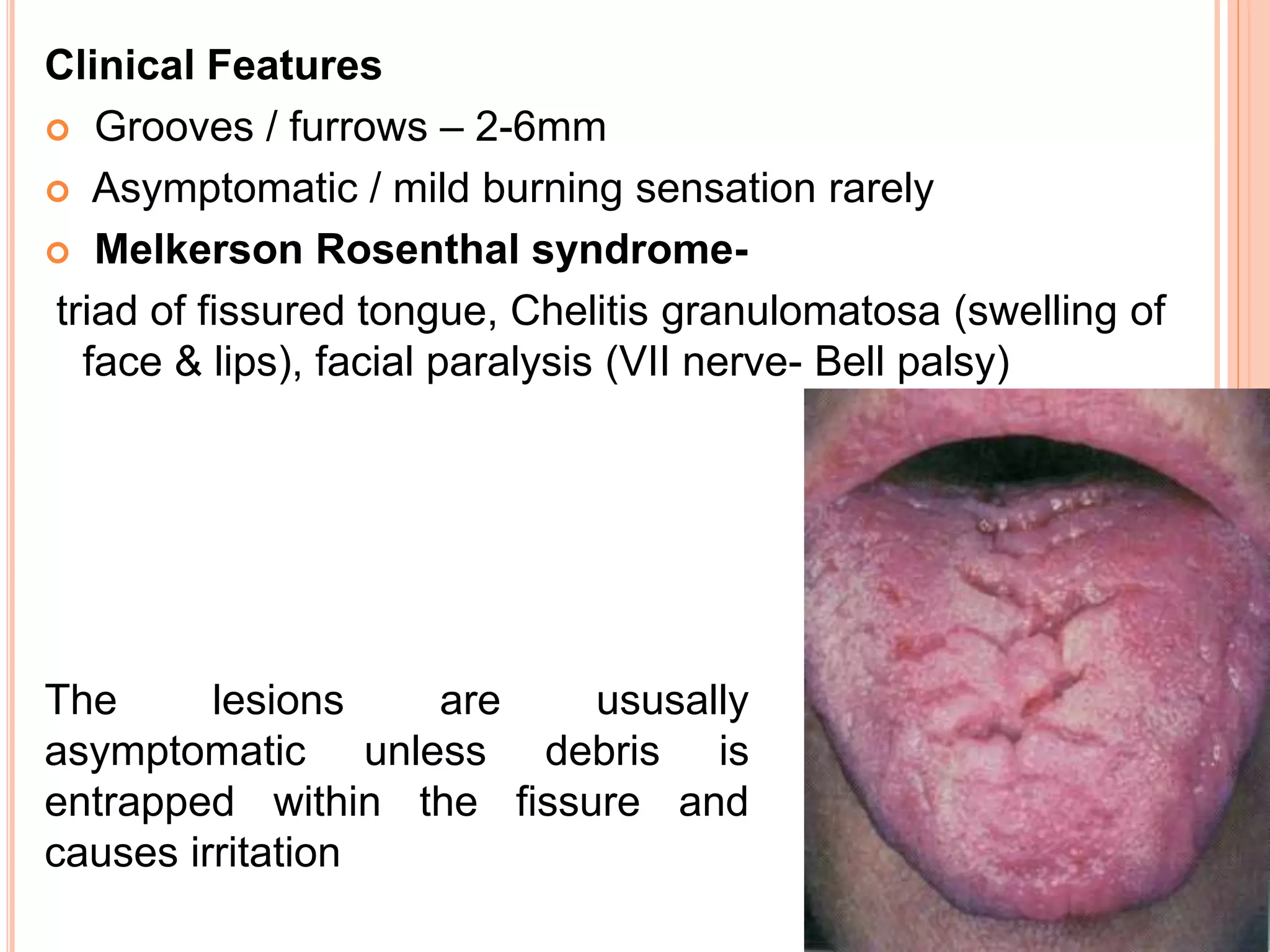

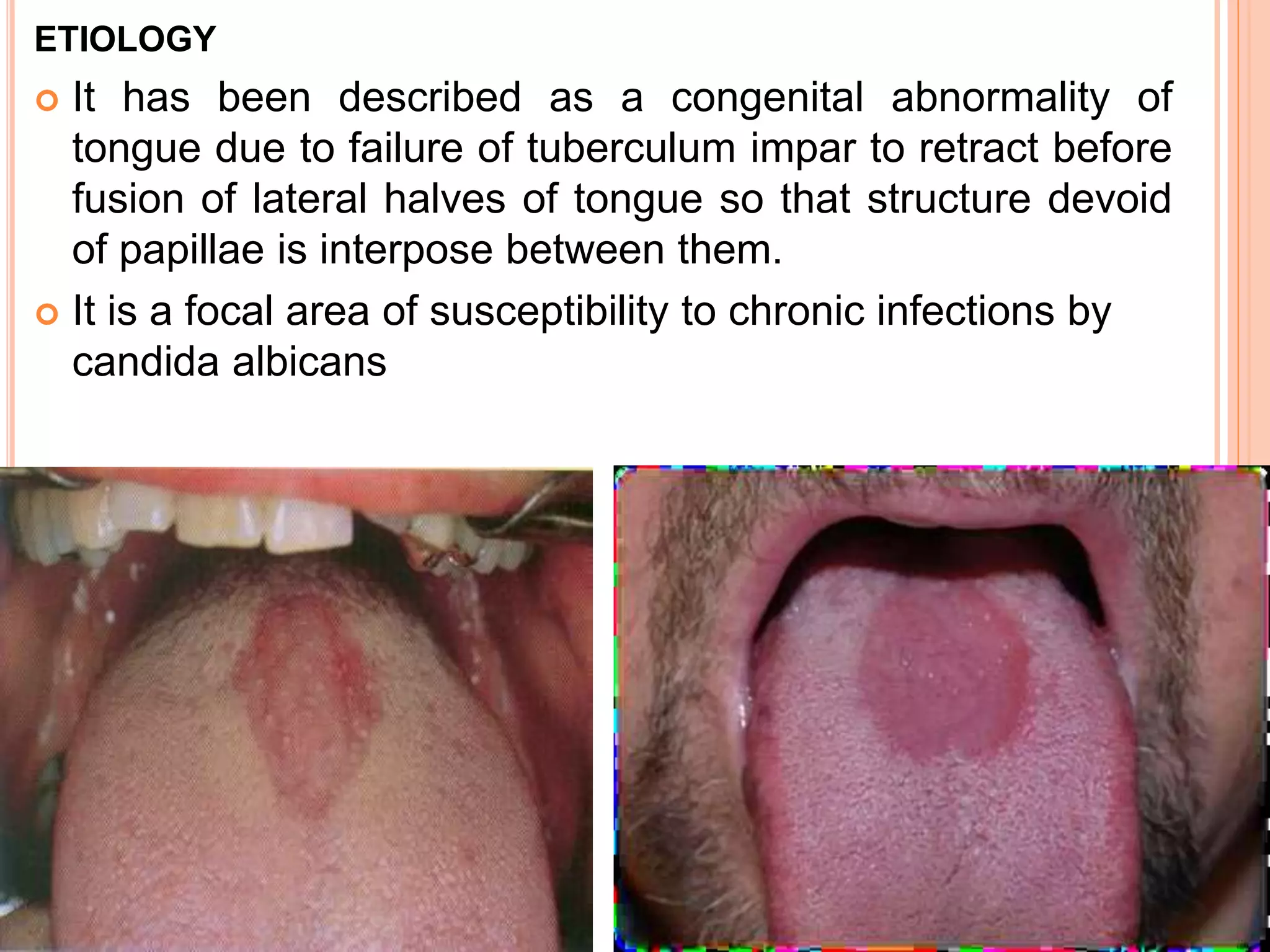



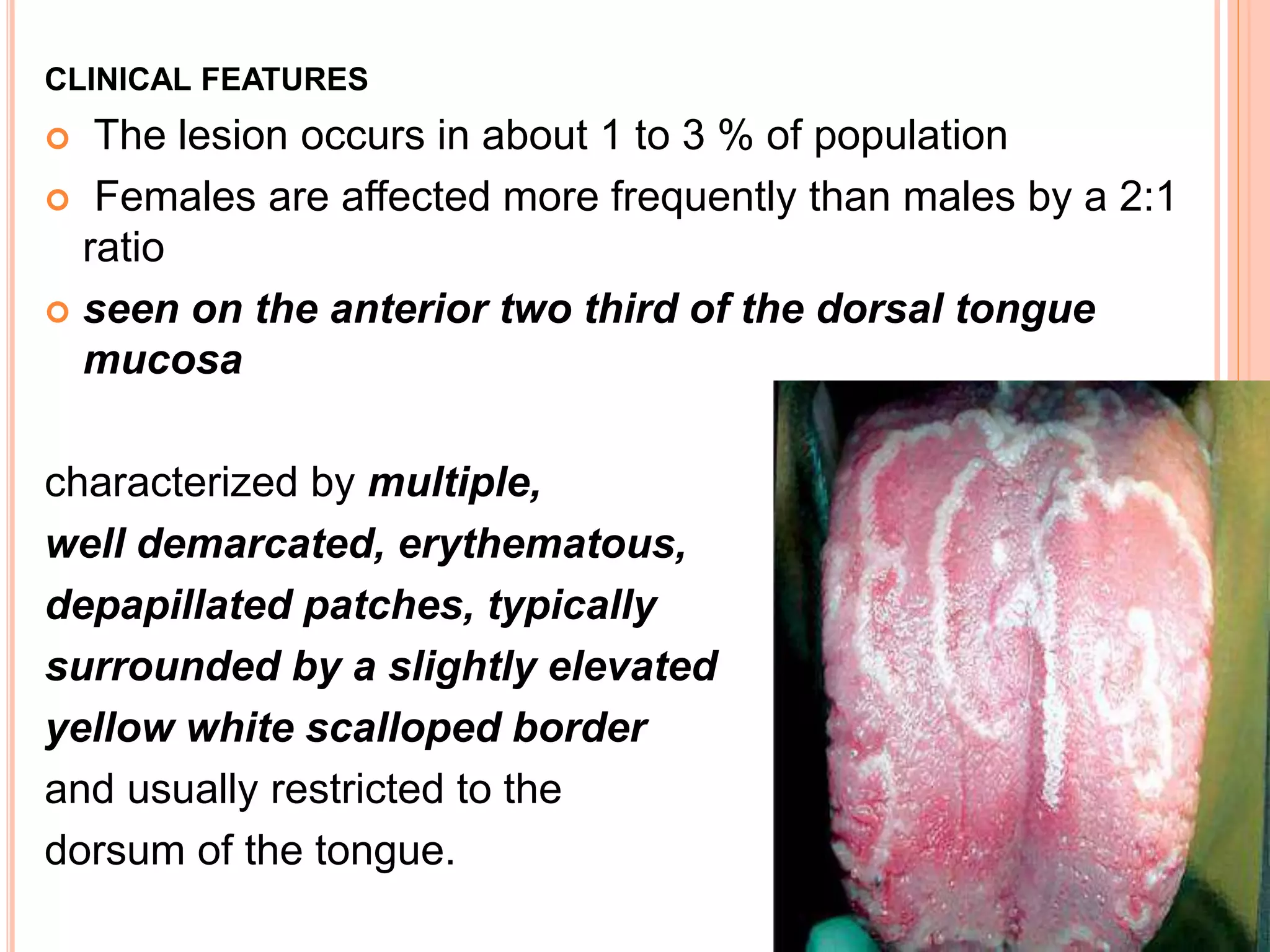

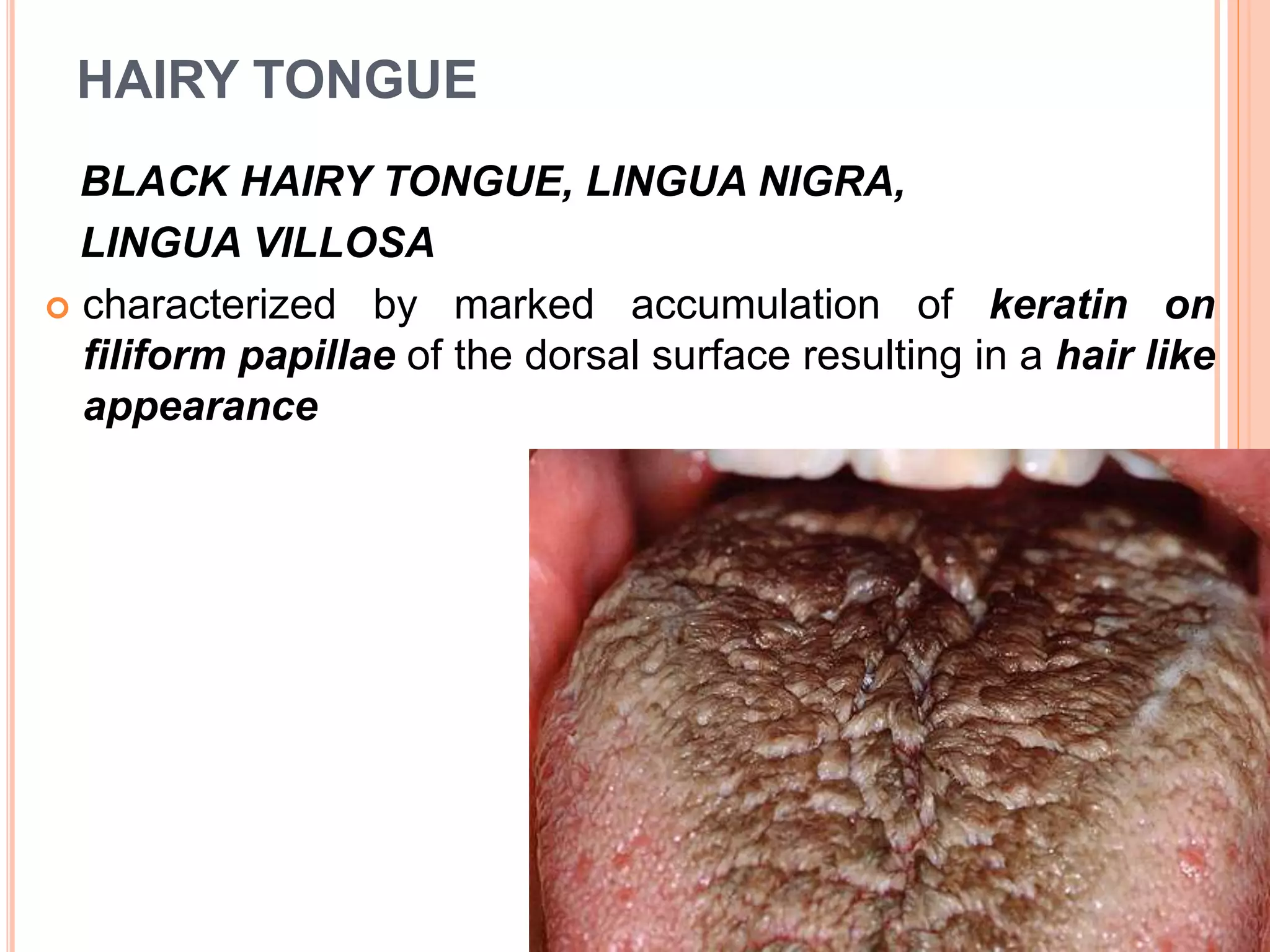
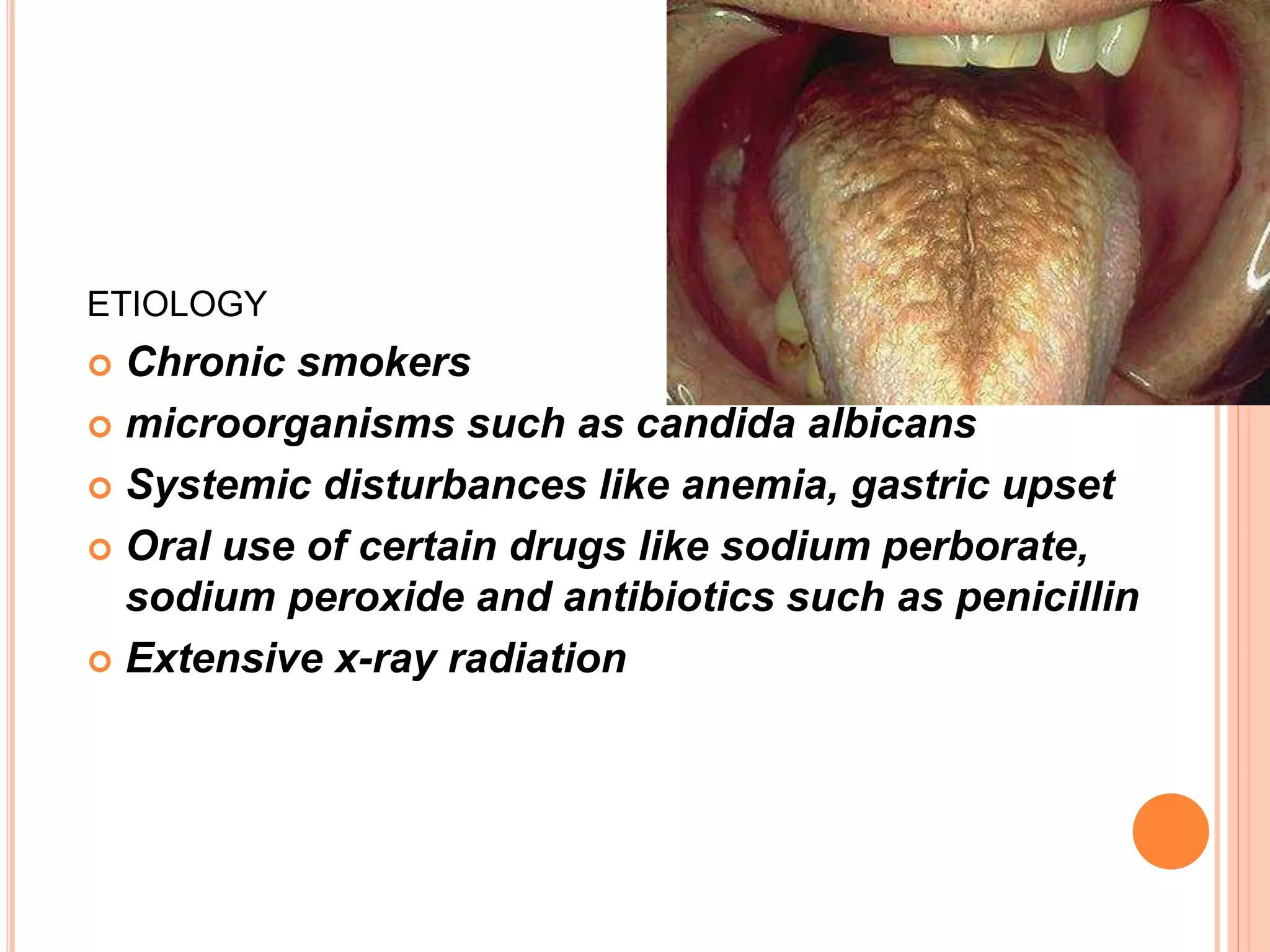

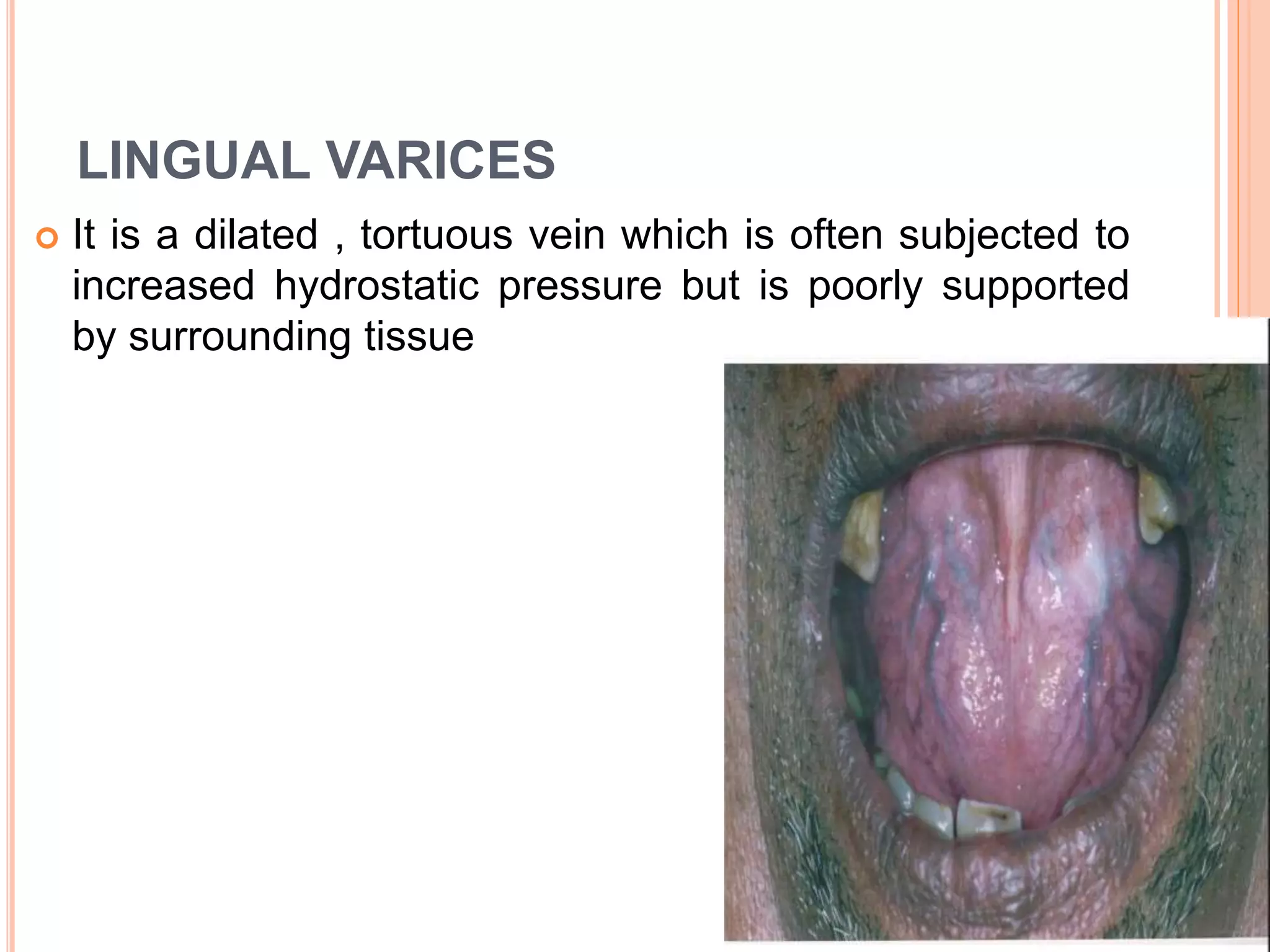
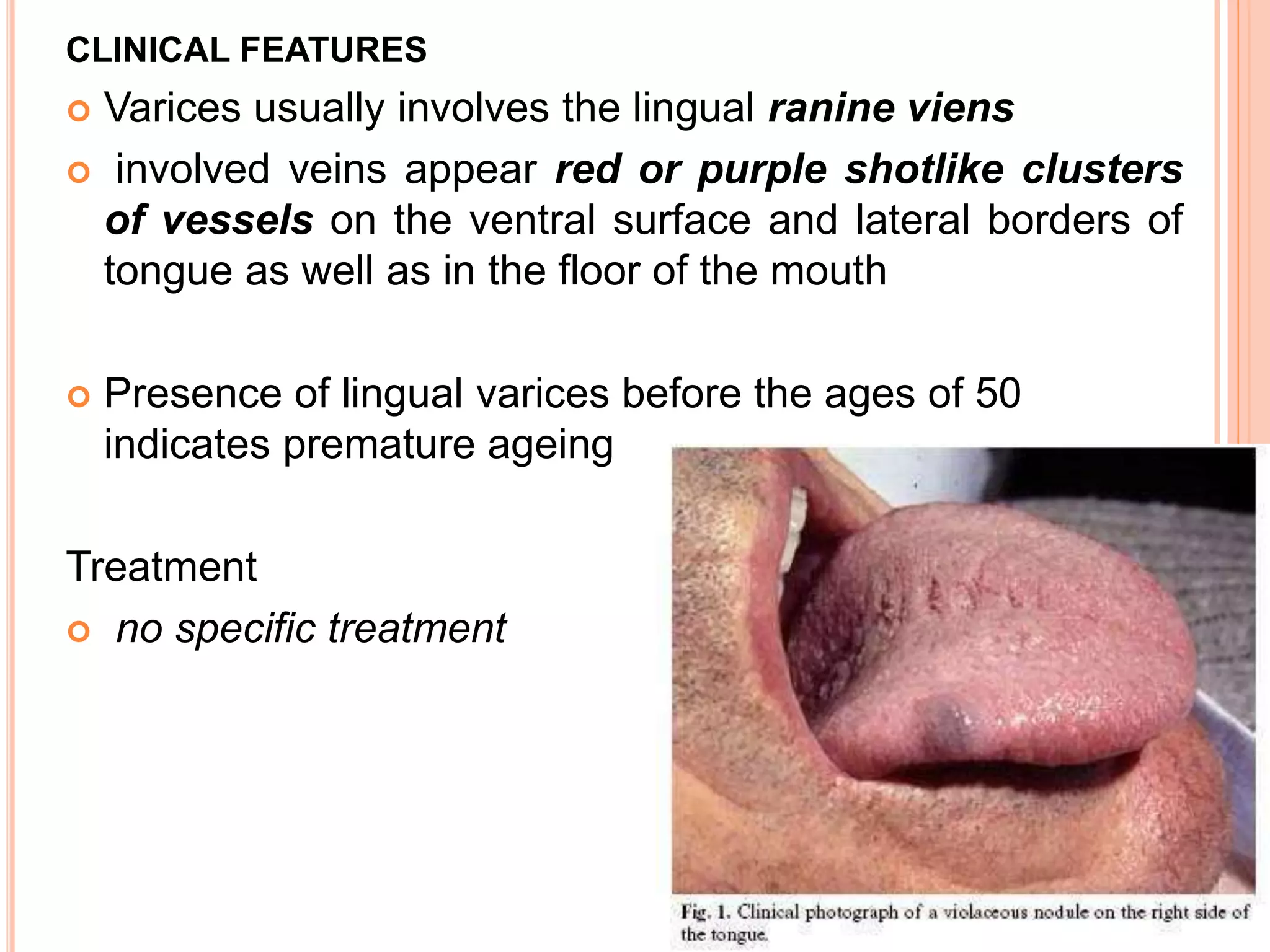

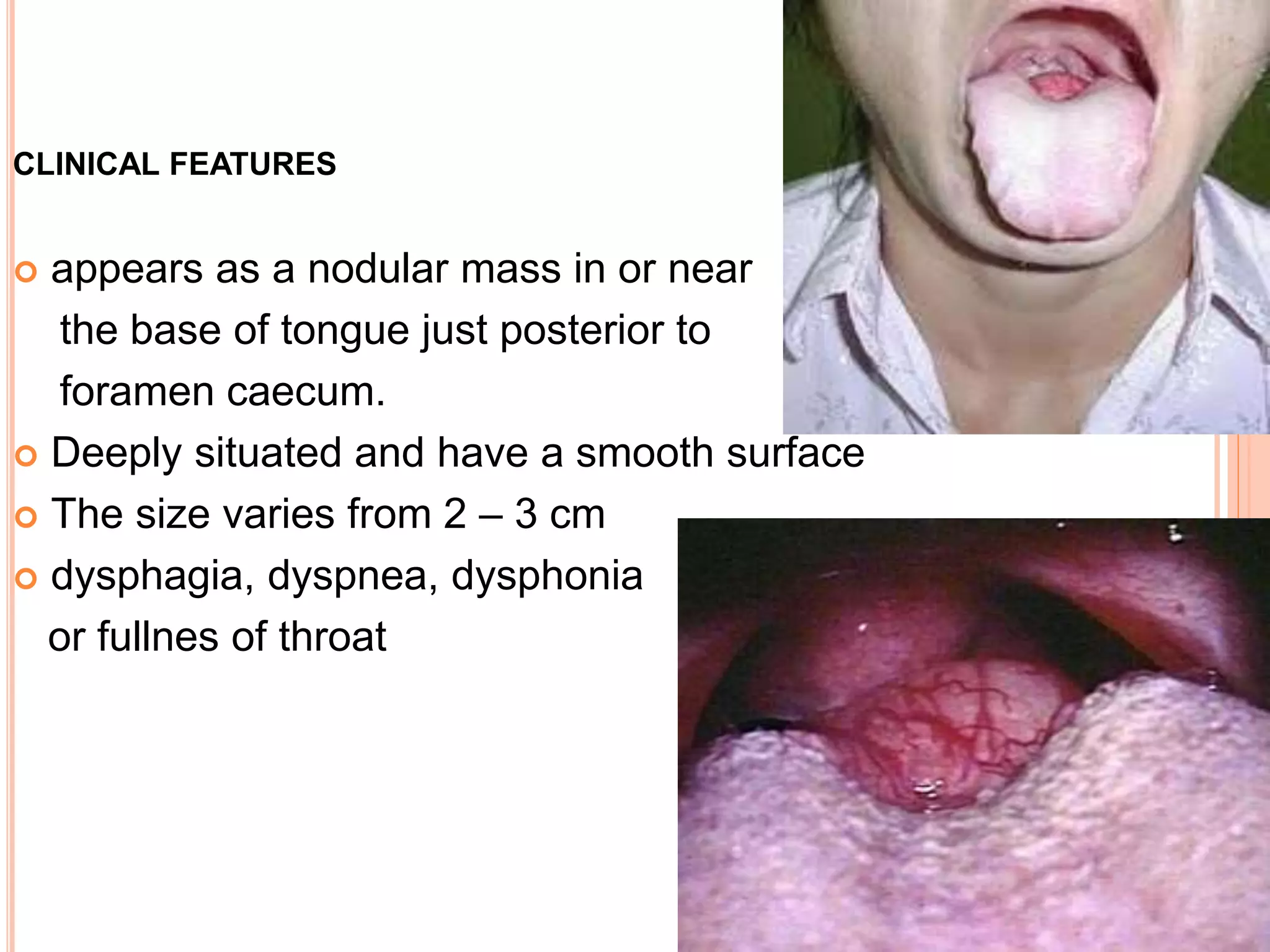




This document discusses various developmental disturbances that can affect the tongue, including microglossia (small tongue), macroglossia (large tongue), ankyloglossia (tongue tie), cleft tongue, fissured tongue, median rhomboid glossitis (reddish patch on dorsal tongue), benign migratory glossitis (geographic tongue), hairy tongue, lingual varices (dilated veins on tongue), and lingual thyroid nodule (thyroid tissue on tongue). Many of these conditions can cause difficulties with speech, swallowing, or irritation of the tongue. Treatment may include surgery, antifungal medications, or thyroid hormone supplements.

















































































