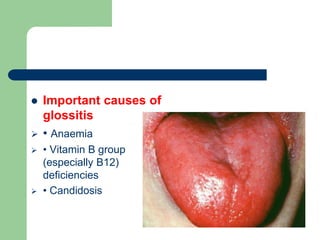
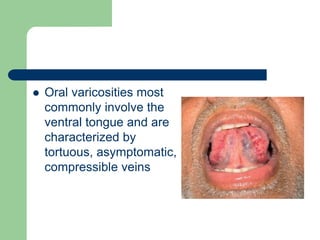
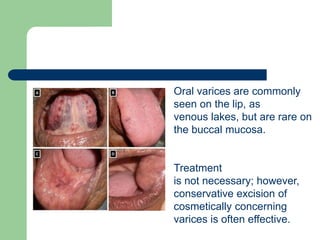
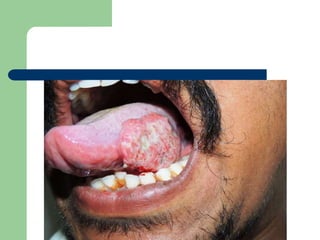
The document discusses various diseases and conditions that can affect the tongue, including glossitis, vascular and lymphatic lesions like infantile hemangiomas and oral varices, infectious conditions like oral hairy leukoplakia and candidiasis, and malignant neoplasms such as squamous cell carcinoma. It provides details on the causes, clinical presentations, and treatments for each condition.