Downloaded 1,649 times



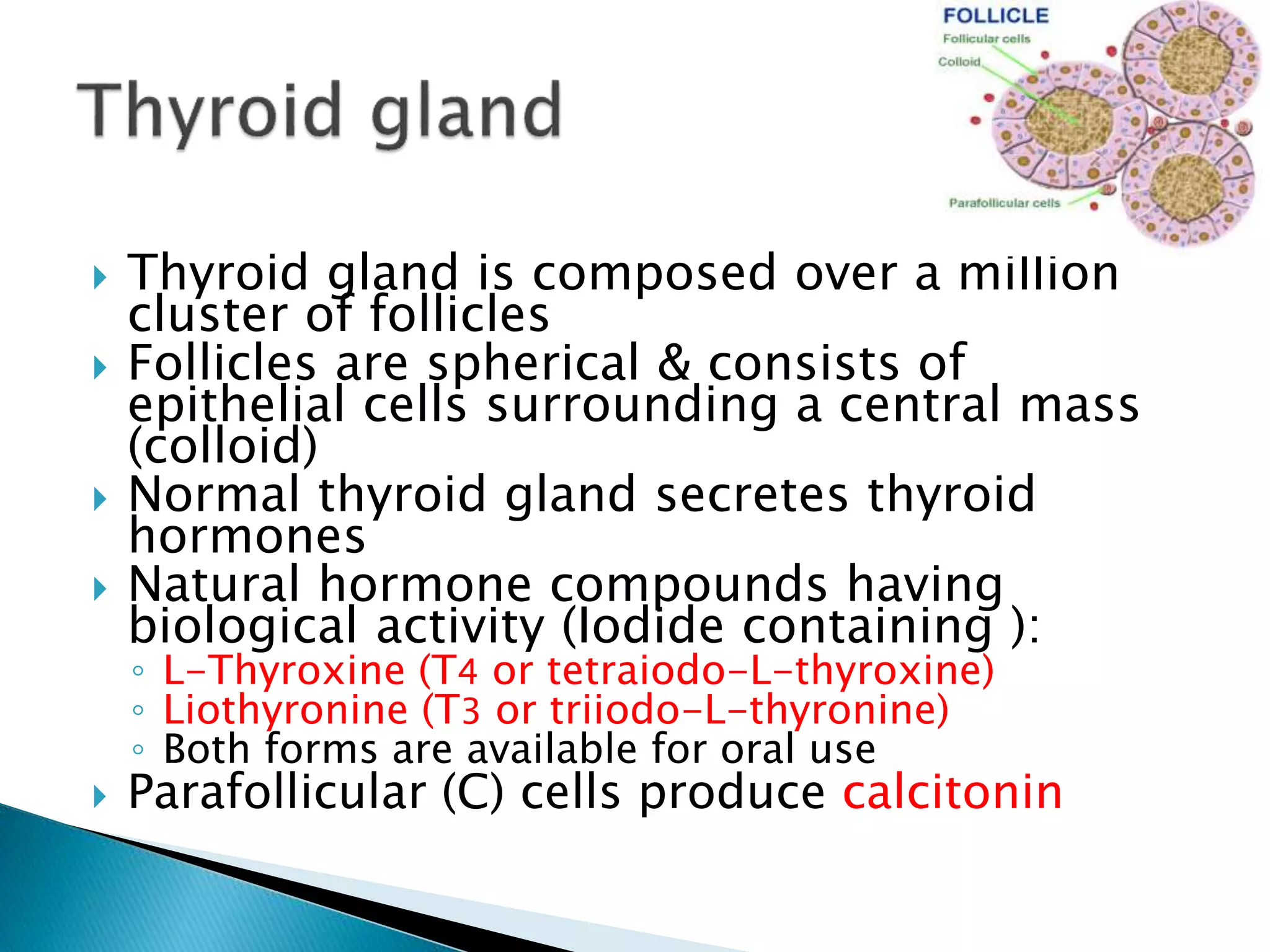





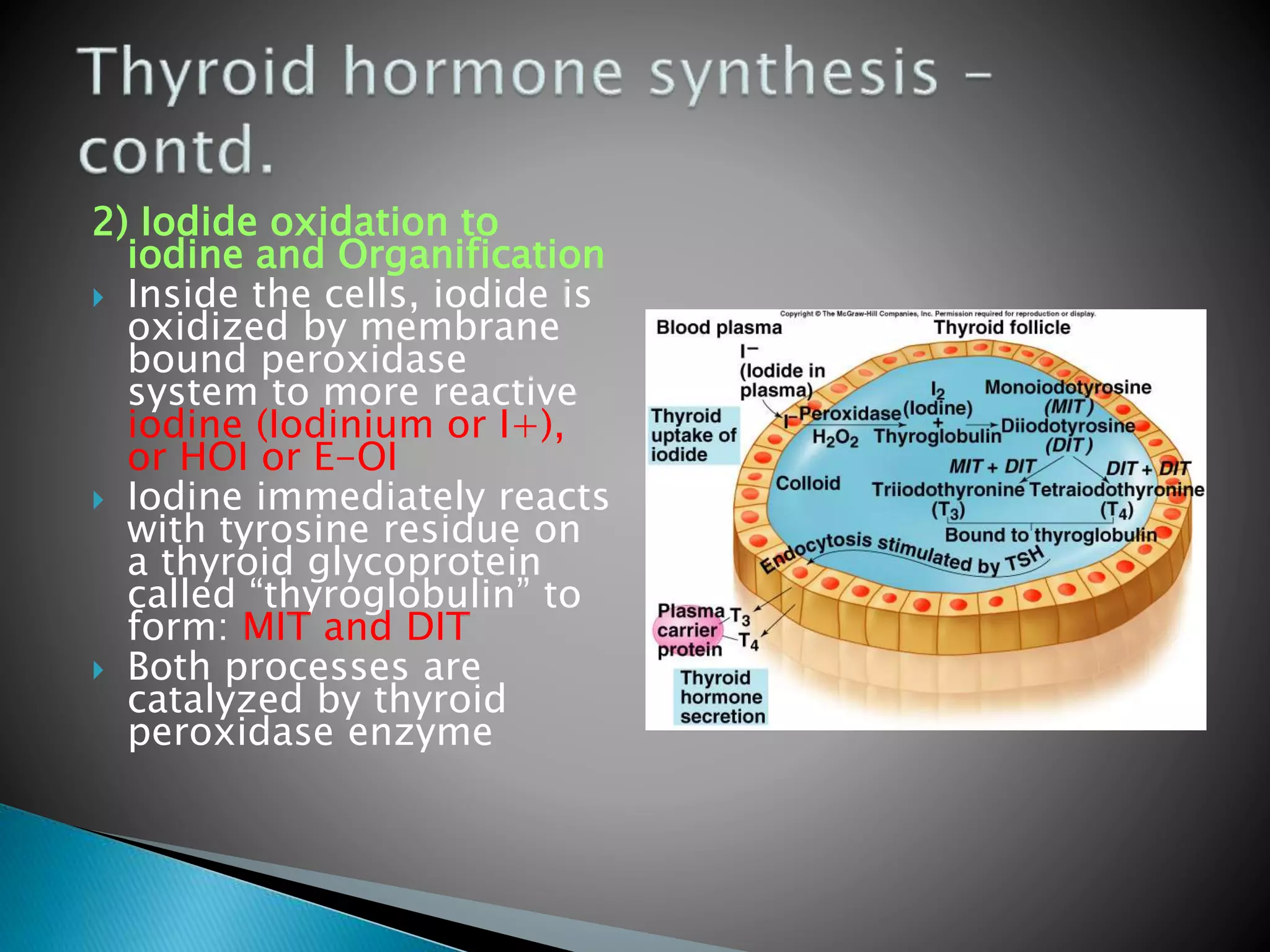


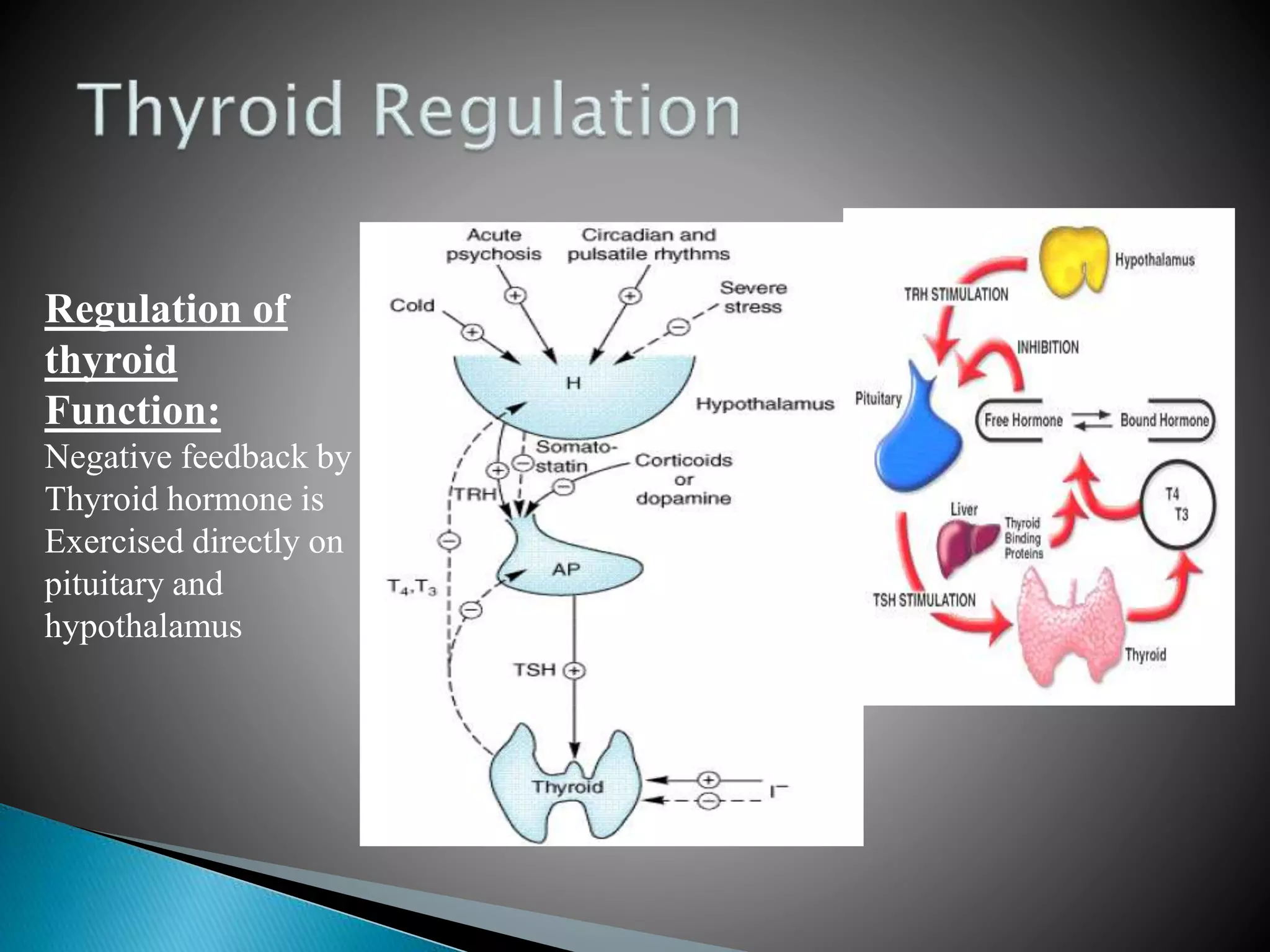


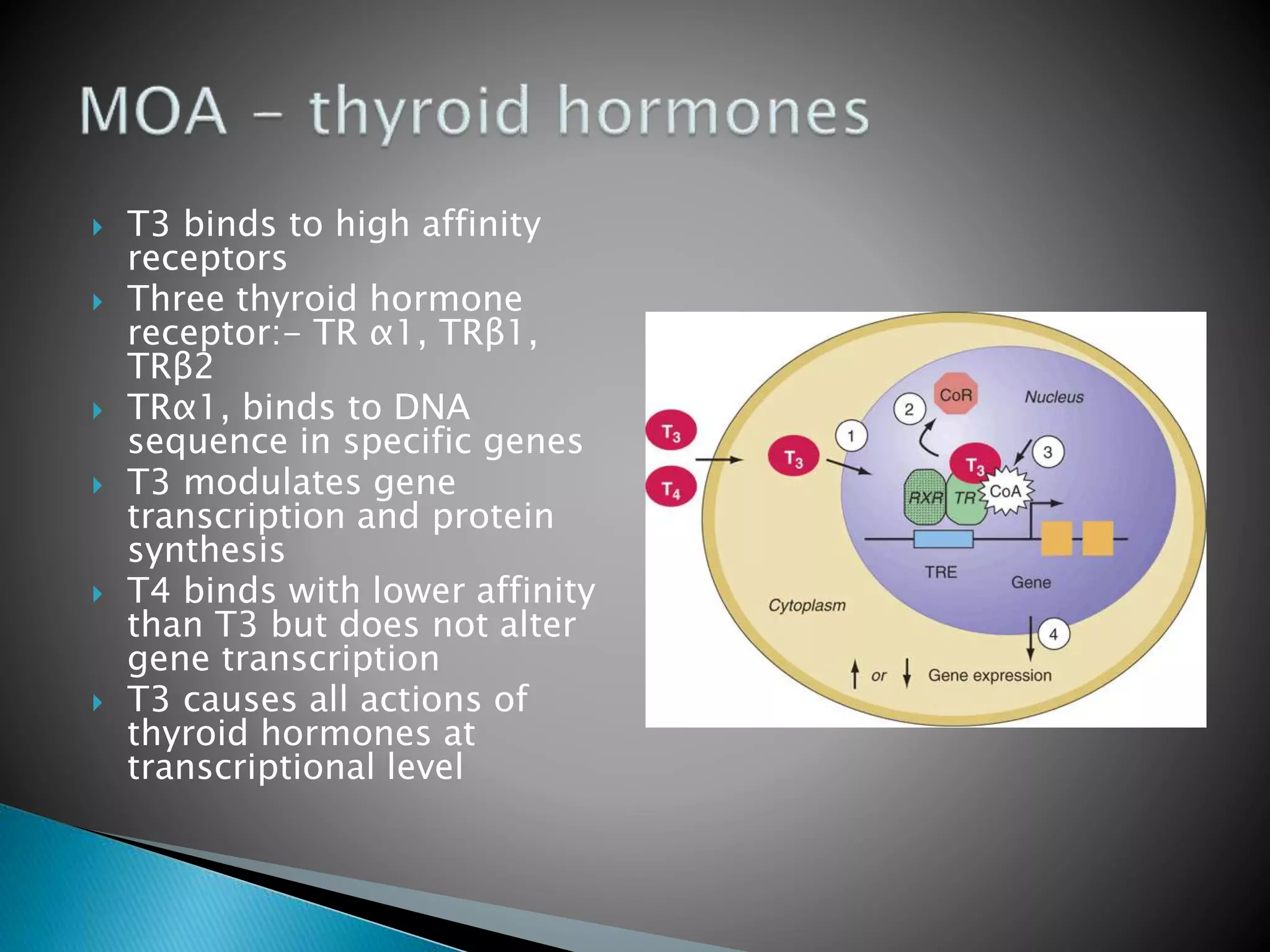






















The document presents a comprehensive overview of thyroid hormones, including their biosynthesis, physiological roles, deficiency states, pharmacology, and therapeutic options for hyperthyroidism and hypothyroidism. It details the mechanisms of hormone synthesis, the metabolism and action of thyroid hormones, as well as the implications of iodine as an essential nutrient. Additionally, it describes treatments for thyroid disorders, such as hormone replacement therapy and the use of antithyroid drugs.








































































































