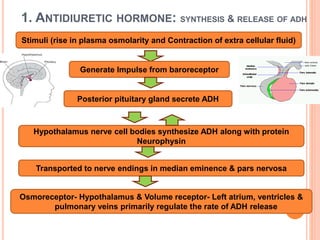
The document provides an overview of antidiuretic agents, primarily focusing on their definitions, classifications, mechanisms of action, pharmacological effects, and clinical uses. It discusses the roles of drugs like vasopressin and its analogs in treating conditions such as diabetes insipidus and bleeding esophageal varices, along with the adverse effects associated with these medications. Additionally, it briefly mentions thiazide diuretics and other supportive agents that complement antidiuretic actions.











































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)











