The document provides an overview of the temporomandibular joint (TMJ), including its anatomy, components, development, function, and age-related changes. Key points include:
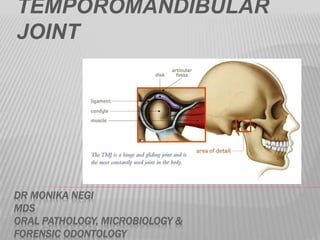
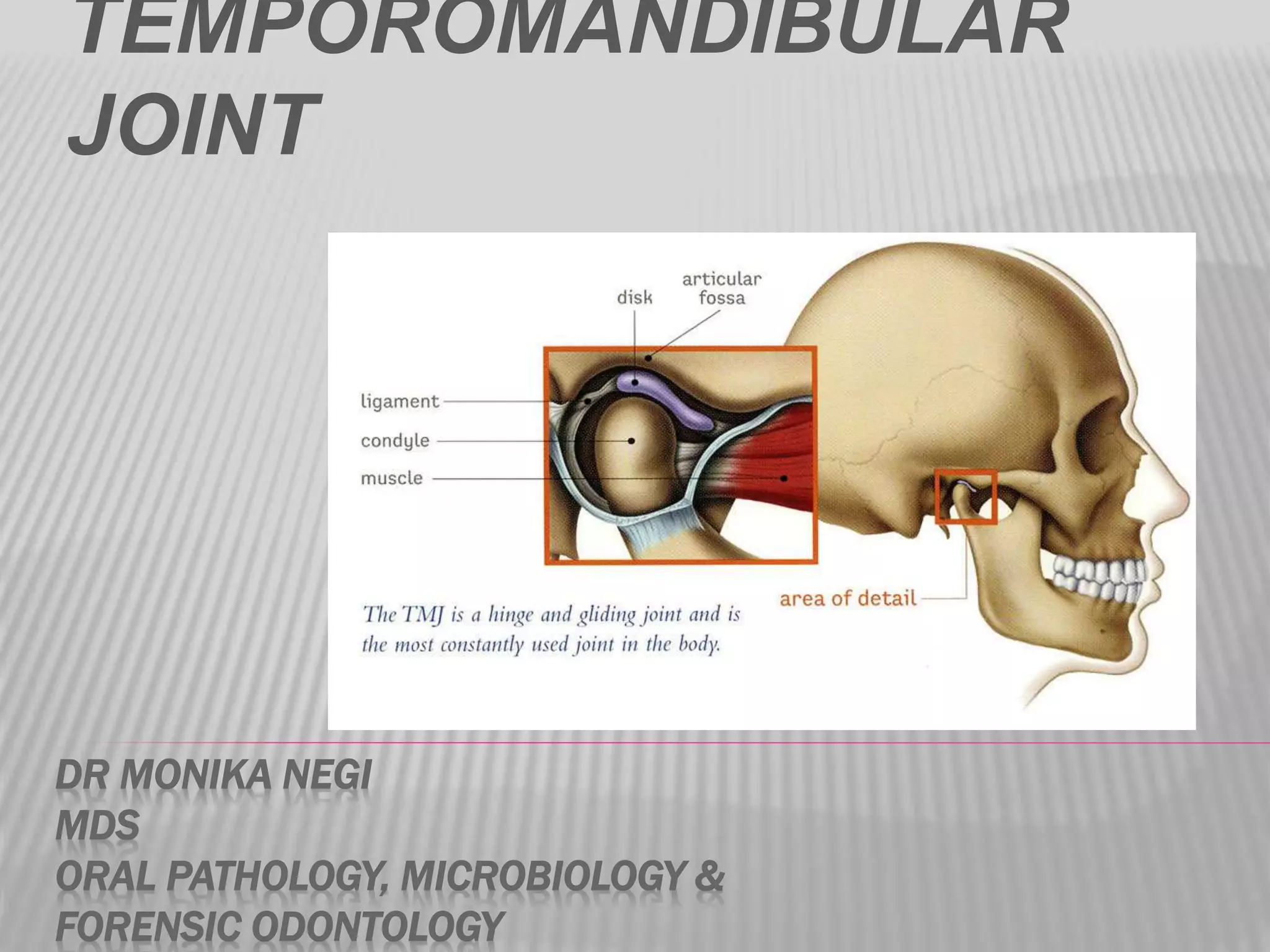
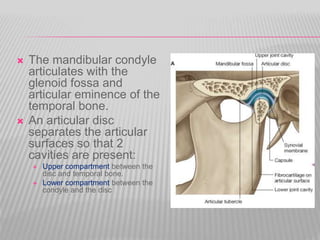
- The TMJ is a synovial joint that permits hinge and gliding movements of the mandible and involves the condyle of the mandible articulating with the temporal bone.
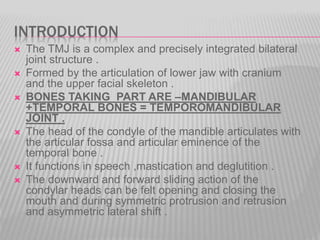
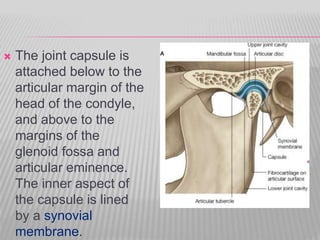
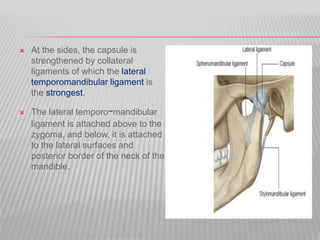
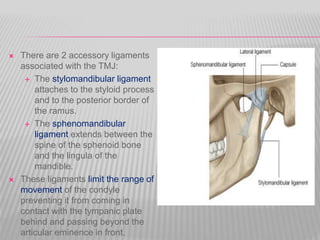
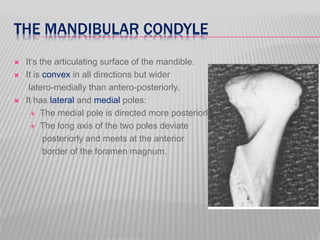
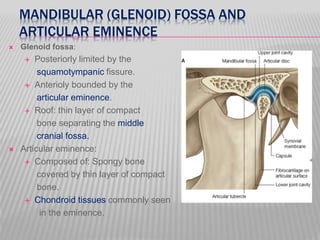
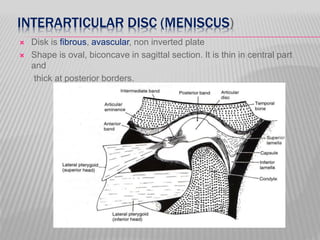
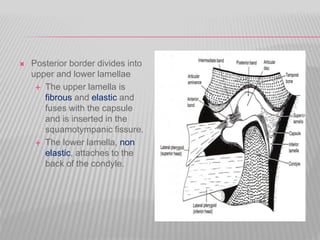
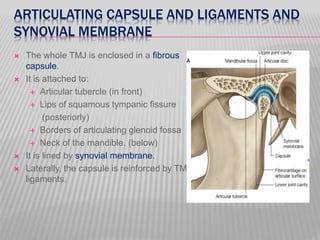
- Its main components are the mandibular condyle, glenoid fossa, articular disc, articular capsule, synovial membrane, and ligaments.
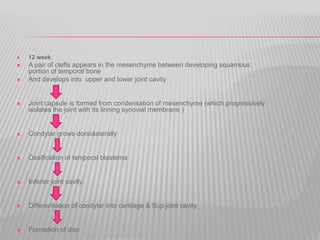
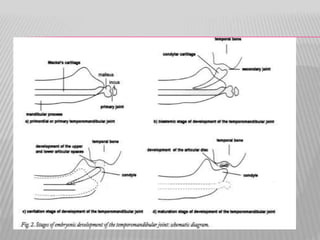
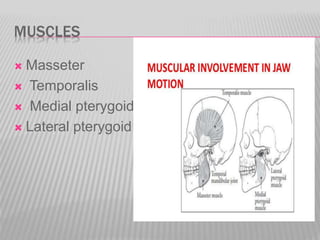
- It develops from Meckel's cartilage and functions in speech, mastication, and deglutition.
- Age-related changes include fl











































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










