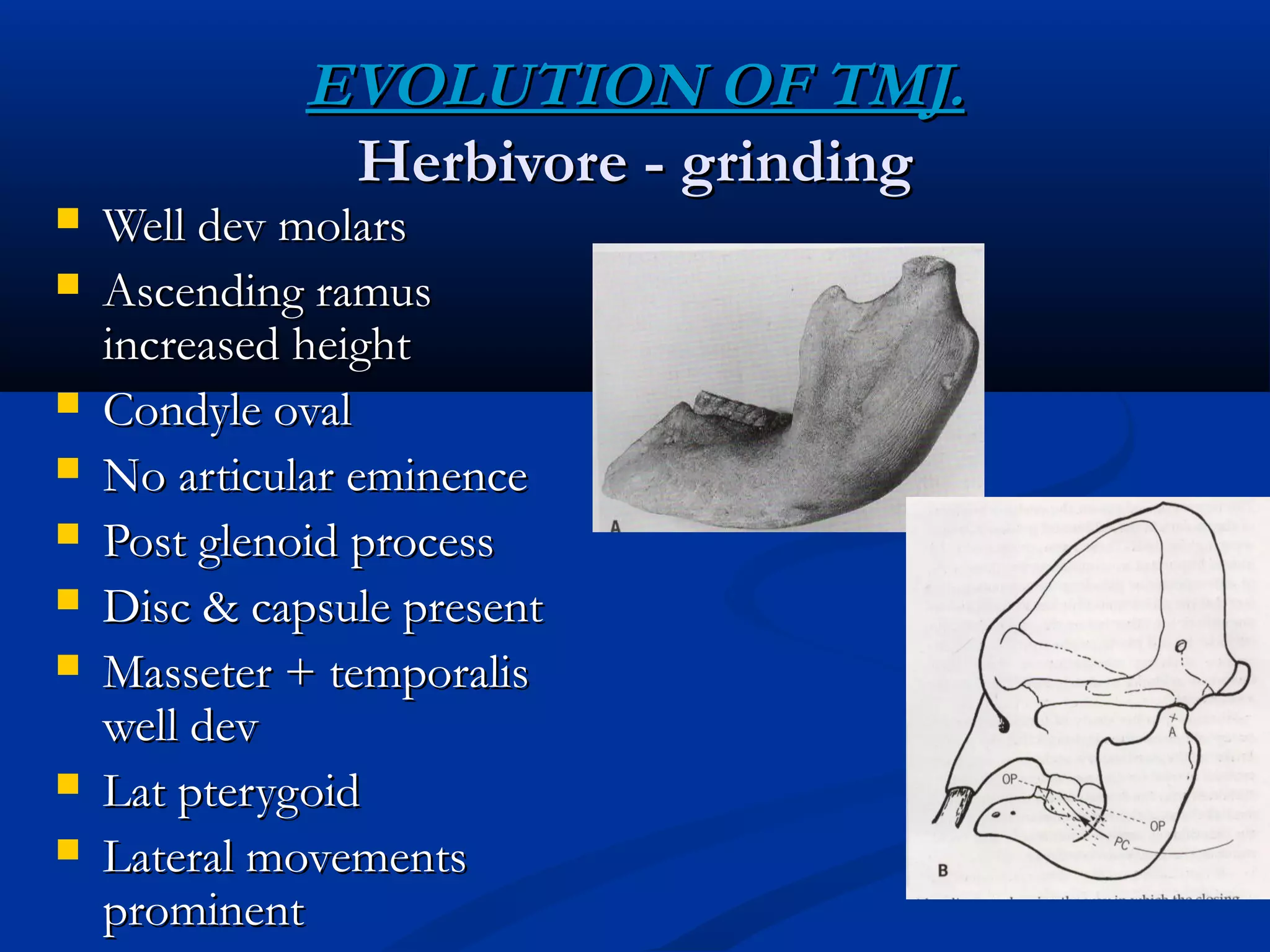
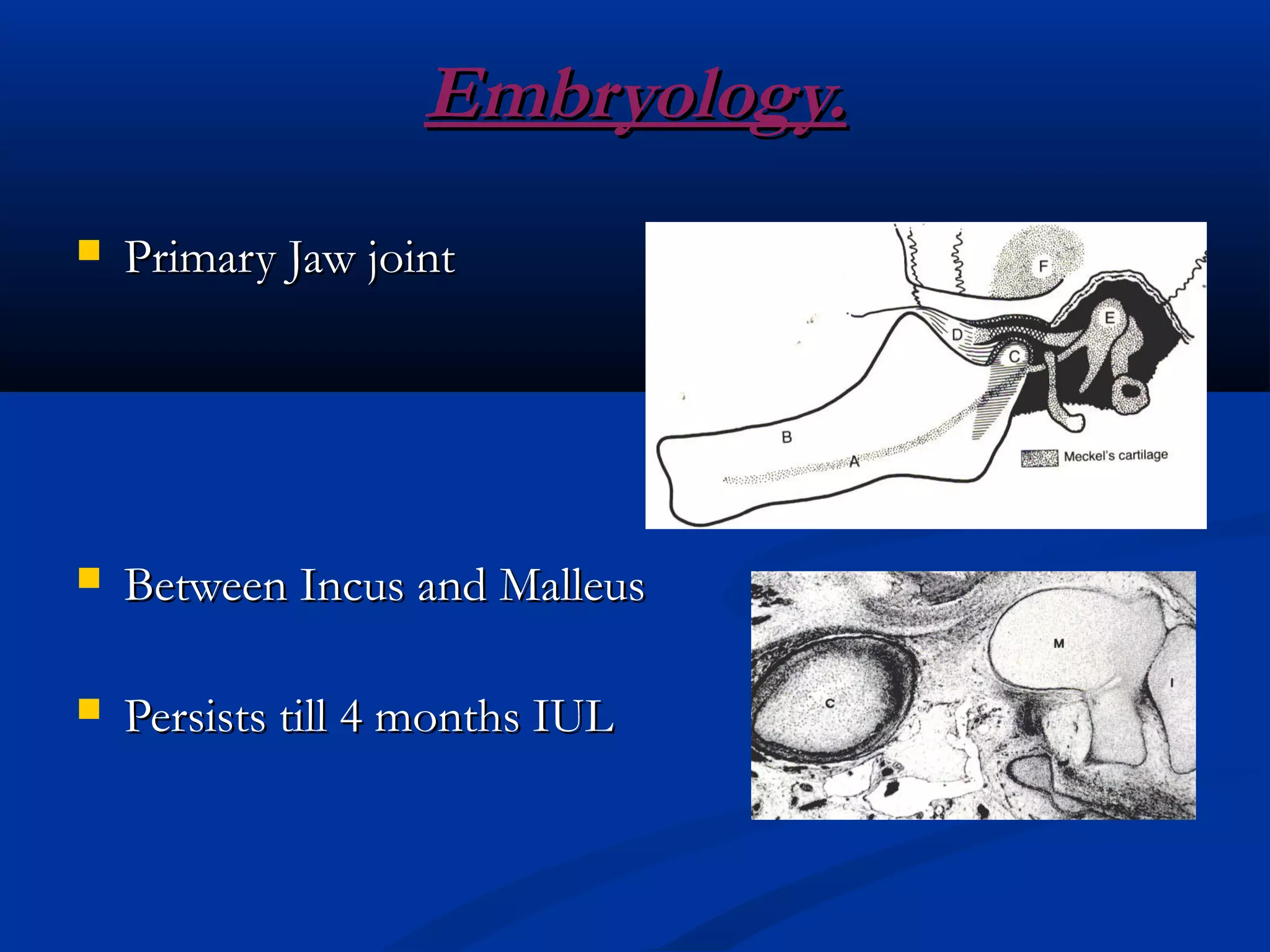
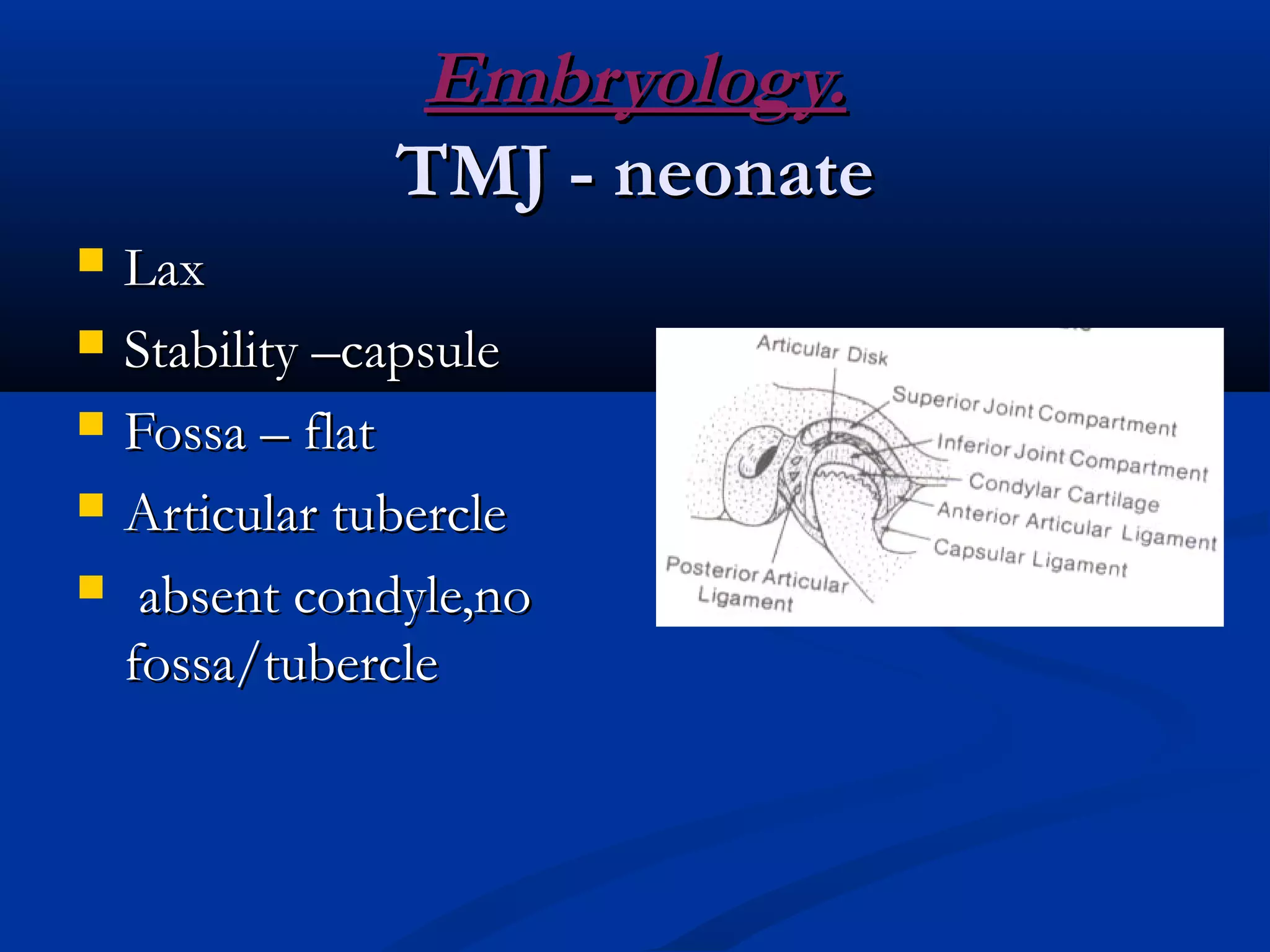
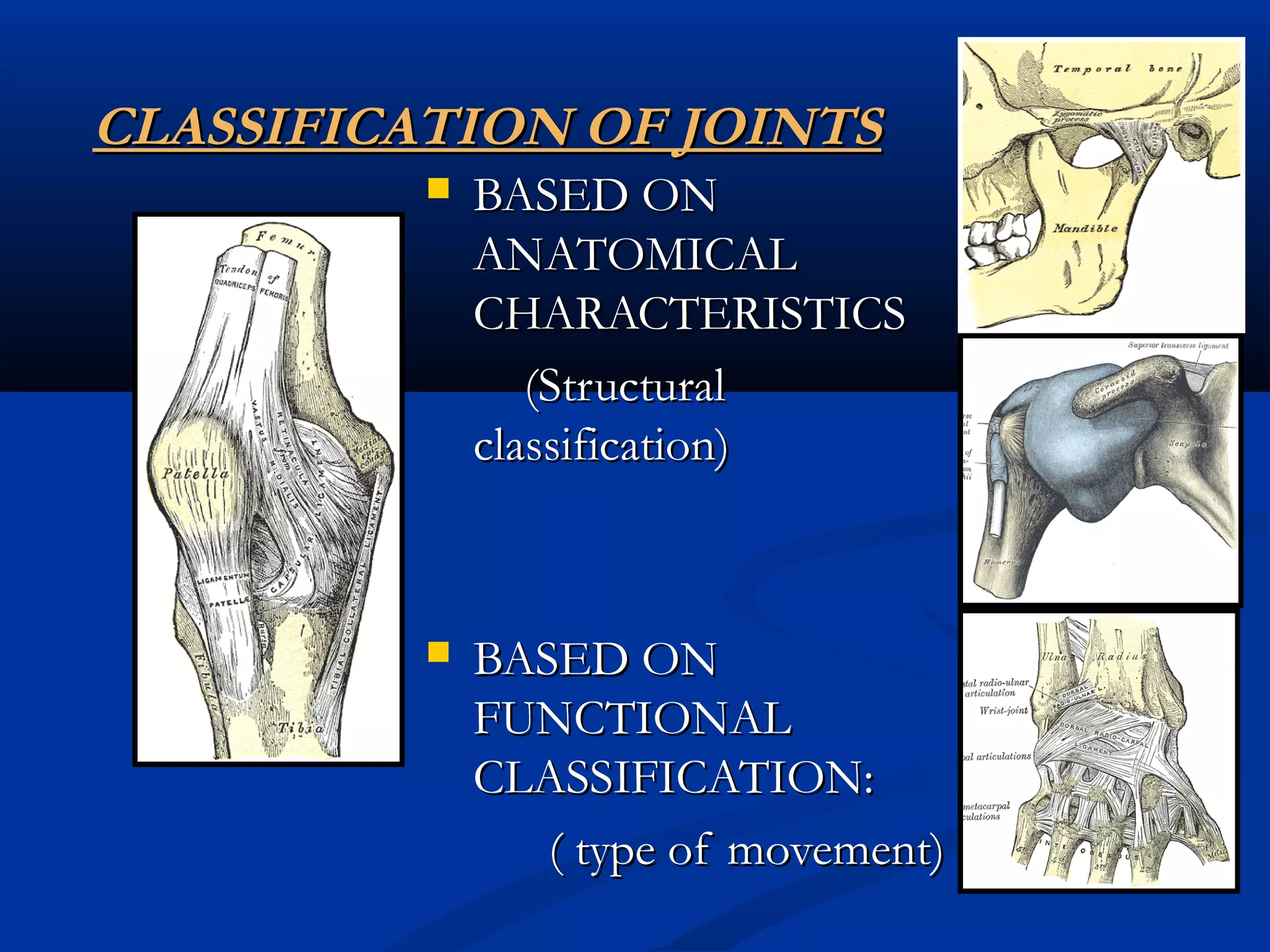
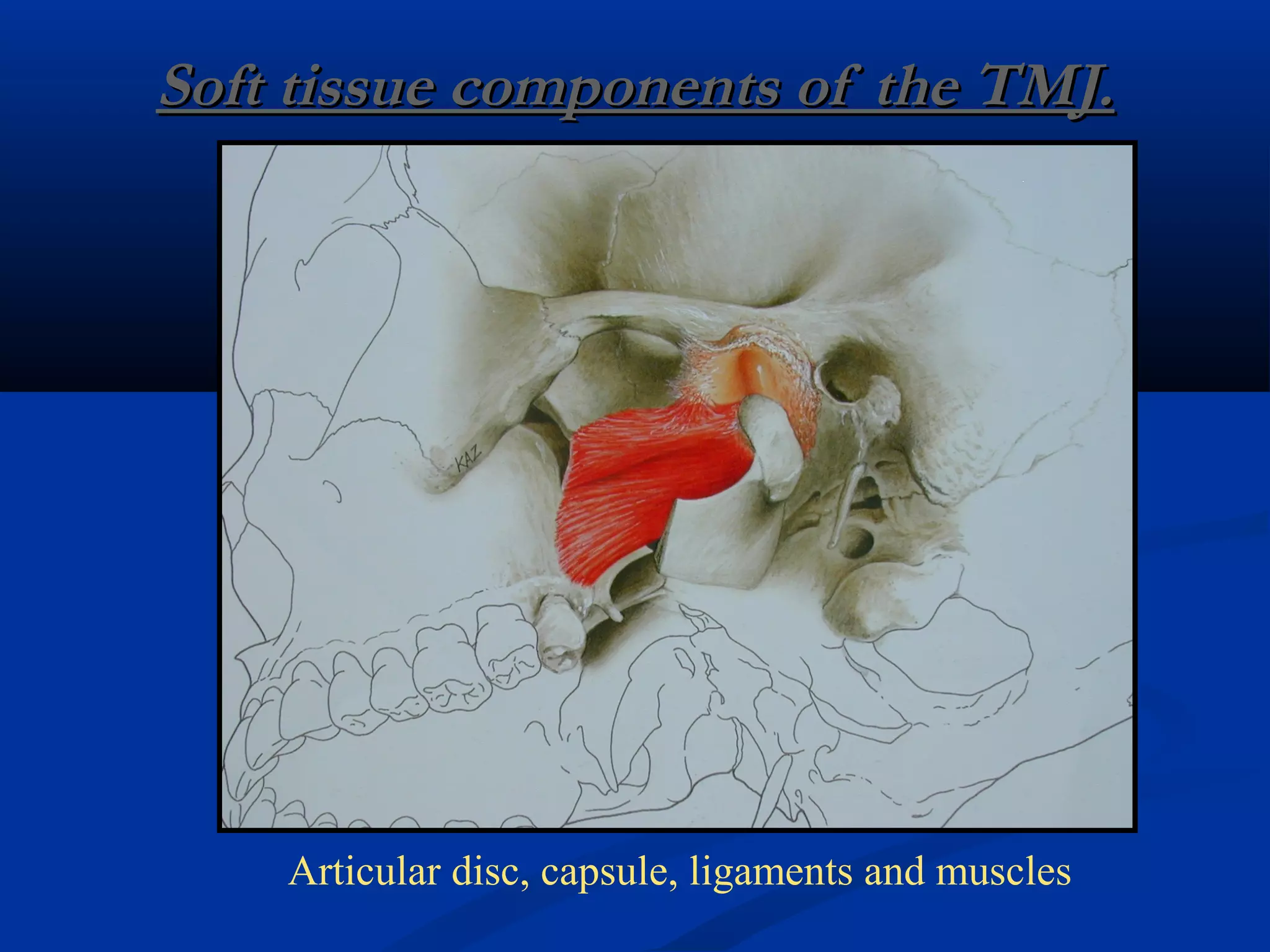
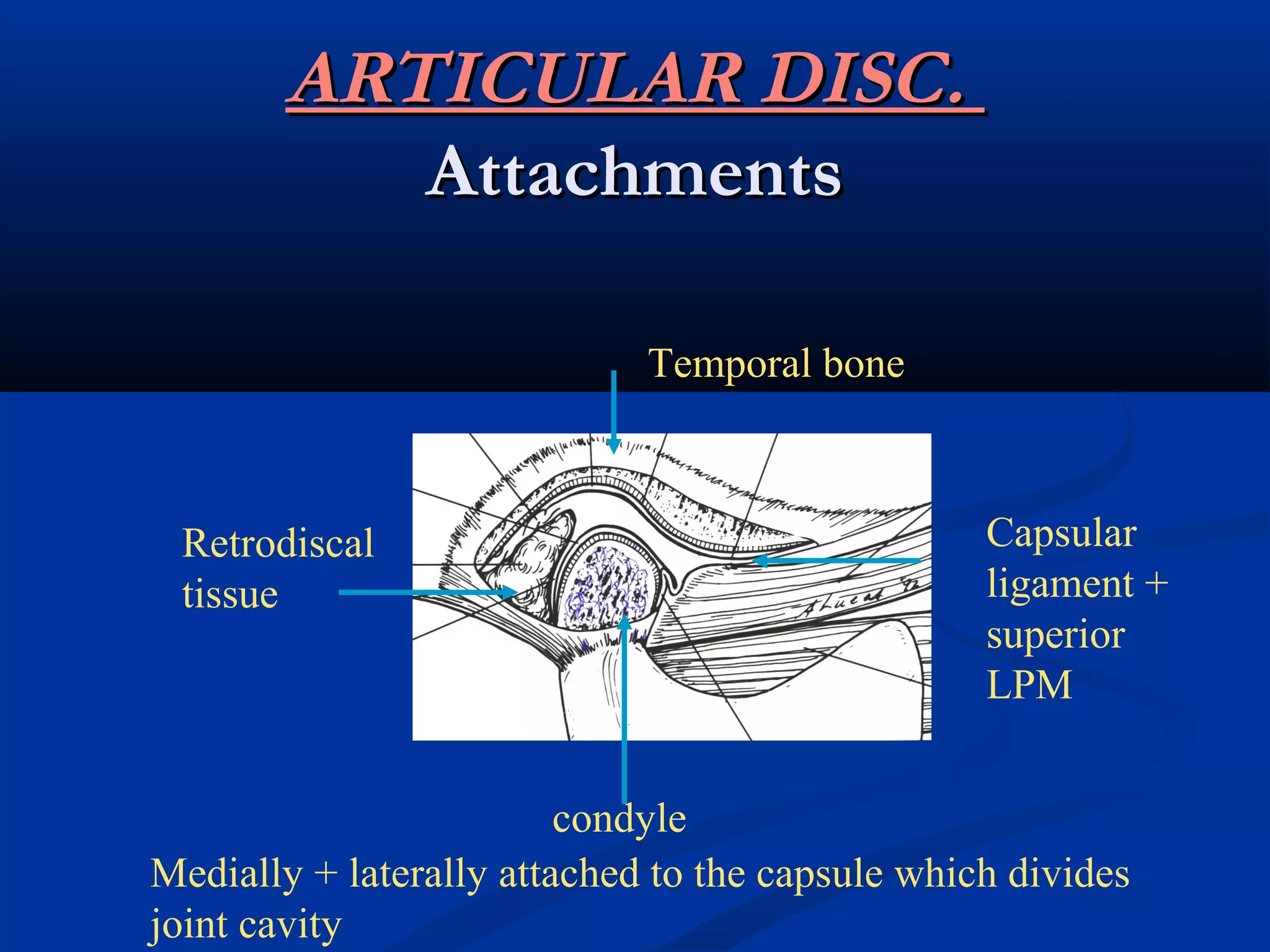
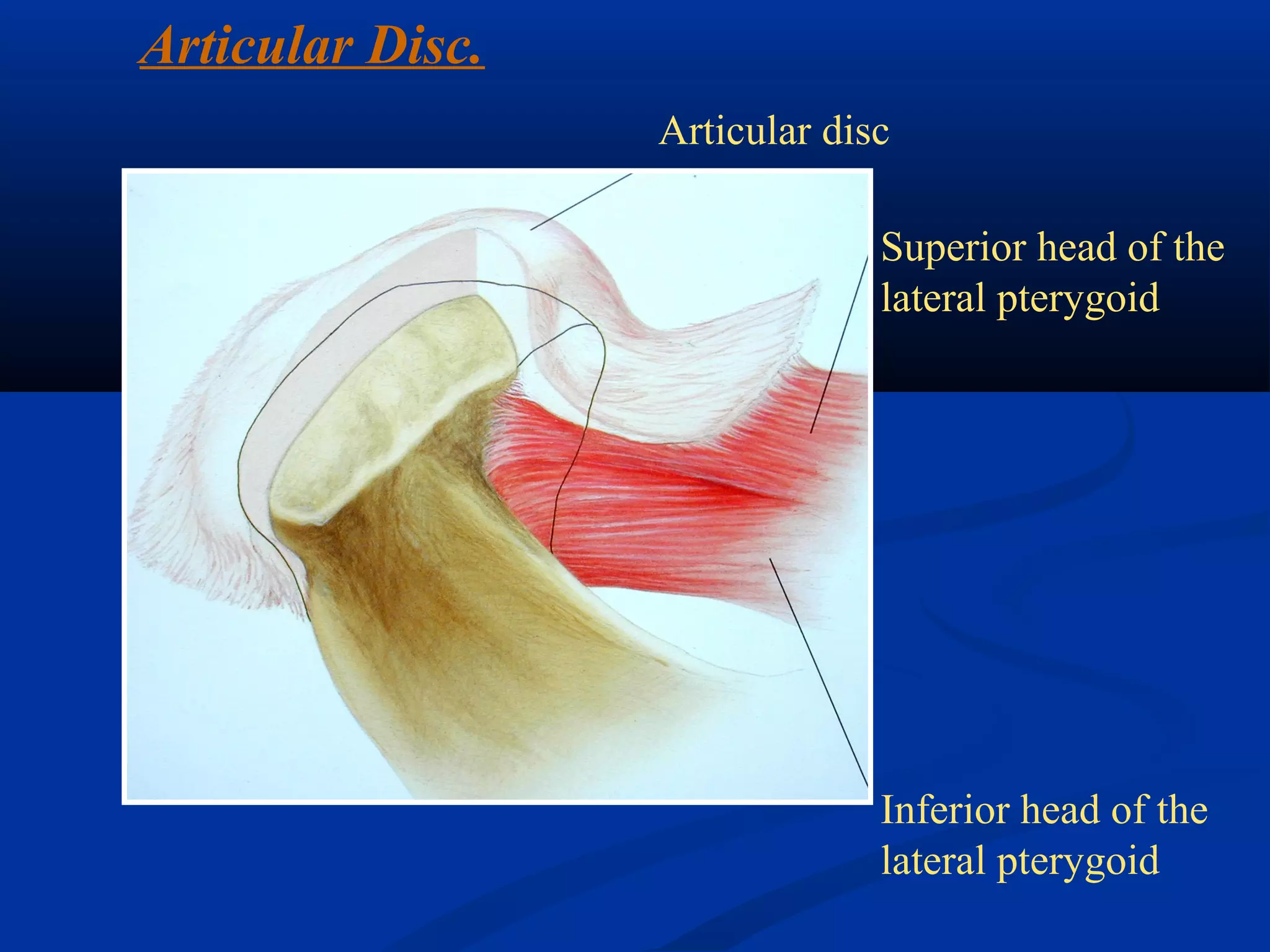
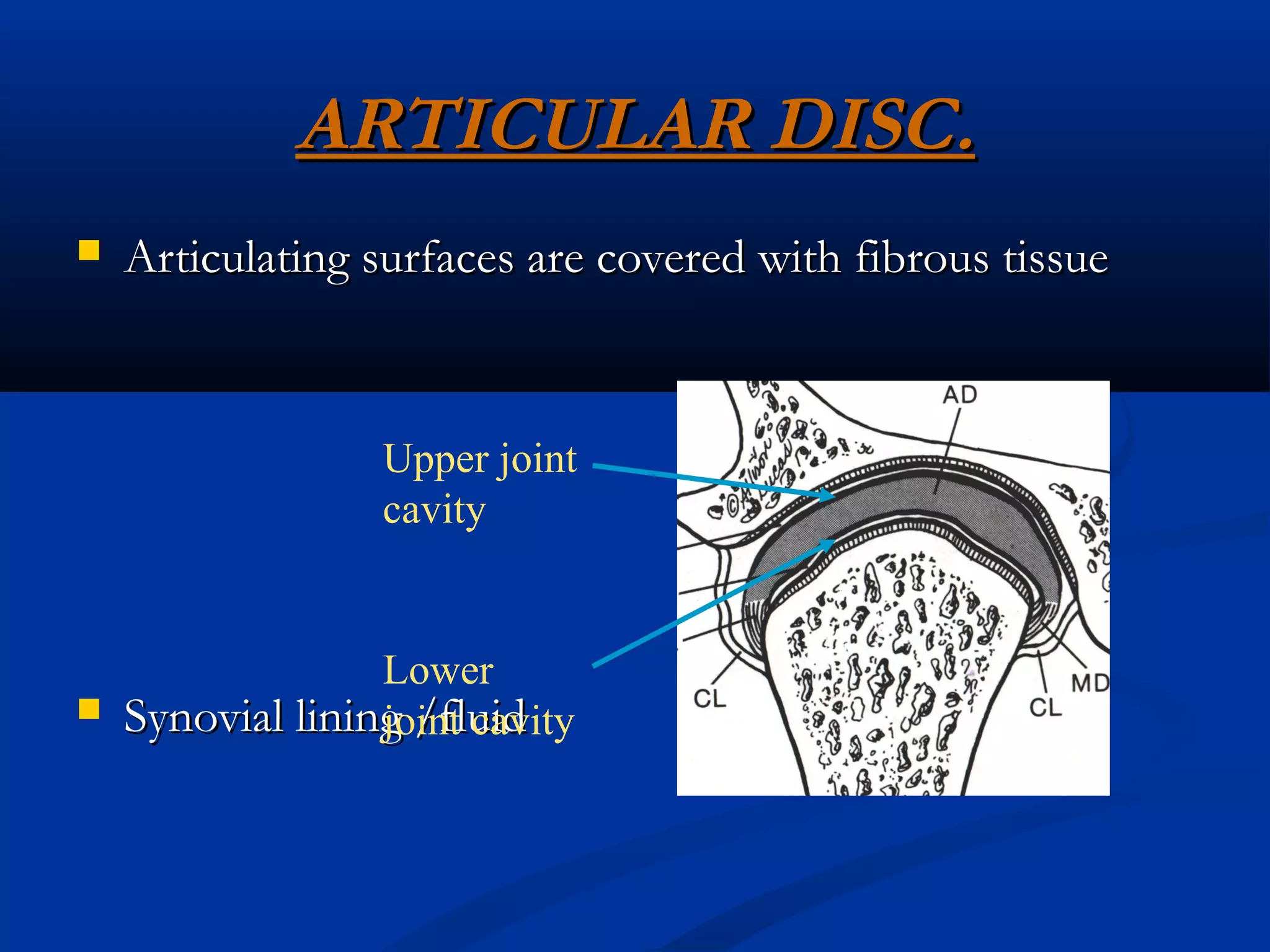
This document provides an overview of a seminar on the development and anatomy of the temporomandibular joint (TMJ). It discusses the evolution of the TMJ from primitive vertebrates to humans. The embryology of the TMJ is described, including the development of the primary and secondary jaw joints. The classification of joints and types of synovial joints are defined. Finally, the key anatomical structures of the TMJ are outlined, including the condylar head, glenoid fossa, articular eminence, muscles of mastication, articular disc, joint capsule, ligaments and blood supply.