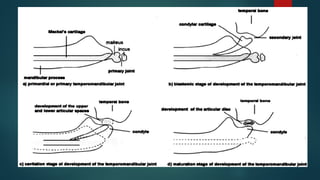
TMJ Development
Thecraniomandibular articulation develops anteriorly to otic
capsule from the first branchial arch mesenchyme.This is early
embryonic joint.
The primary embryonic joint formed by joining malleus and incus
which develops from first branchial arch.This serve as the primary
TMJ upto 16 week of prenatal life.
By the end of 7-11 week of gestation the secondary TMJ begins to
develop.
At about 9 week a condensation of mesenchyme appears
surrounding the upper posterior surface of rudimentary ramus.
5.
This masschondrifies at about 10-11 week to form cartilagineous
mandibular condyle with progressive endochondral ossification. The
cartilage fuses with posterior part of bony mandibular body.
At about 9-10 weeks the muscle fibres becomes more
differentiated.Blood vessels and nerve can be seen at 10 week of
gestation.
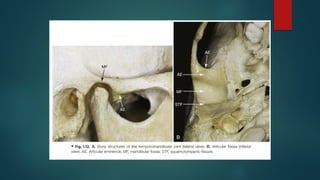
The appearance of mandibular fossa is seen earlier than condyle at
about 7-8 weeks.
7.
0ssification offossa continues and at about 22 weeks fossa shows
both medial and lateral walls and articular eminence is evident.
The differentiating mesenchymal cells interposed between condyle
and fossa gives raise to capsular and intercapsular structures of TMJ.
Articular disc first seen at about 7th
week,by 10th
week first sign of
collagenous fibres within disc develops and becomes prominent by
12 week.
8.
From 19to 20th
week the disc increasingly takes on its
fibrocartilaginous composition.At this stage only disc shows pattern
of differential cell proliferation in which central region becomes
thinner than periphery.
Articular capsule first appears at 9-11 week.By 17th
week capsule is
seen with fully formed tissue boundary between intracapsular and
extracapsular components of TMJ.
Temporomandibular Joint
Thearea where the mandible articulates with the
temporal bone .
Also known as Ginglymoarthrodial joint as it
provides for both hinging and gliding
movements.
The TMJ is formed by the mandibular condyle
fitting into mandibular fossa of temporal bone.
Separating these two bones from direct
articulation is the articular disc.
12.
ARTICULAR DISC
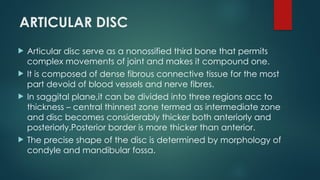
Articulardisc serve as a nonossified third bone that permits
complex movements of joint and makes it compound one.
It is composed of dense fibrous connective tissue for the most
part devoid of blood vessels and nerve fibres.
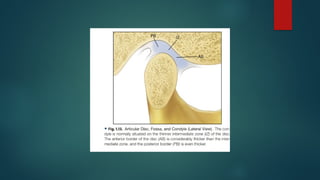
In saggital plane,it can be divided into three regions acc to
thickness – central thinnest zone termed as intermediate zone
and disc becomes considerably thicker both anteriorly and
posteriorly.Posterior border is more thicker than anterior.
The precise shape of the disc is determined by morphology of
condyle and mandibular fossa.
14.
During movement discis somewhat flexible
and can adapt to functional demands of the
articular surfaces .
Disc maintain its morphology unless destructive
forces or structural changes occur in joint
If these changes occur,morphology gets
irreversibly altered producing biomechanical
changes during function.
15.
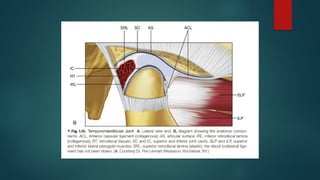
Attachments of articulardisc
Posteriorly it is attached to RETRODISCAL TISSUE made up of loose
connective tissue that is highly vascularized and innervated
Superior retrodiscal lamina attach the articular disc posteriorly to
tympanic plate.
Inferior retrodiscal lamina attach inferior border of posterior edge
of disc to posterior margin of articular surface of the condyle .
The superior and inferior attachments of the anterior region of disc
are to capsular ligament.
Superior attachment is to anterior margin of articular surface of
temoral bone.
16.
Inferior attachmentis to anterior margin of articular surface of
condyle .
Anteriorly between the attachments of capsular ligament disc is
also attached by tendinous fibres to superior lateral pterygoid
muscle.
18.
Synovial Membrane
Theinternal surface of cavities are surrounded by
specialized endothelial cells that form a synovial
lining ,this along with specialized synovial fringe
located at anterior border od retrodiscal tissues
producing synovial fluid.
BOUNDARY lubrication – occurs when joint is moved
Synovial fluid located in border or recess area is
forced on articular surface ,thus providing
lubrication
19.
WEEPING Lubrication– during function of joint forces are created
between articular surfaces which drives a small amount of synovial
fluid in and out of articular tissues.
Under compressive forces ,synovial fluid released and eliminates
friction in the compressed but not moving joint.
Synovial fluid act as a medium for providing for providing metabolic
requirements to these tissues along with lubricant between articular
surfaces and mimimize the friction .
Free and rapid exchange exists betwwn vessels of capsule synovial
fluid and the articular tissues.
20.
Histology of Articularsurfaces
Articular cartilage of TMJ is very different from typical one as it form
from intramembranous cartilage rather than from endochondrial
ossification .
Because of that, the articular fibrocartilage of TMJ keeps its chondro
progenitor cells buried deep within it
The zones of TMJ fibrocartilage are set up differently , which allows
for continued TMJ growth repair and remodelling.
22.
Articular cartilageis composed of chondrocytes and intercellular
matrix.
Chondrocytes produce the collagen,proteoglycans,glycoproteins
and enzymes that form the matrix.
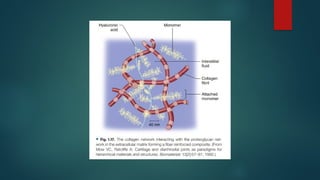
Proteoglycans are complex molecules composed of a protein core
and glycosamineoglycan chaims. They are connected to a
hylauronid acid chain forming proteoglycan aggregates which are
hydrophilic and tends to bind water , the matrix expands and
tension in collagen fibres counteracts the swelling pressure of
proteoglycan aggregates.
24.
In thisway interstitial fluid contributes to support joint loading .
The external pressure from joint loading is in equilibirium with the
internal pressure of articular cartilage ‘
As loading increases,tissue fluid flows outward until a new
equilibirium is achieved.
As loading decreases,fluid is reabsorbed and the tissue regain its
original volume.
25.
Innervation of TMJ
Branchesof mandibular nerve mostly
the Auriculotemporal nerve provides
both motor and sensory inervation .
Additonal innervation is provided by –
deep temporal nerve
massetric nerve
26.
Vascularizatiom of TMJ
Predominant vessels are
superficial temporal artery from posterior
middle meningeal artery from anterior
internal maxillary artery from inferior
Other arteries are
deep auricular
Anterior tympanic
Ascending pharyngeal
27.
LIGAMENTS
Ligaments donot enter actively into joint
fumctiom but instead act as passive restraining
devices to limit and restricts border movements.
Made up of connective tissue gibres that have
particular lengths and do not stretch .
If extensive forces applied to these , can be
elongated ,it compromises the function of
ligament altering joint function.
28.
Three functional ligamentssupports TMJ –
the collateral ligament
the capsular ligament
the temoporomandibular ligament
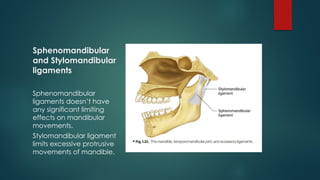
Two accessory ligaments –
the sphenomandibular
the stylomandibular
29.
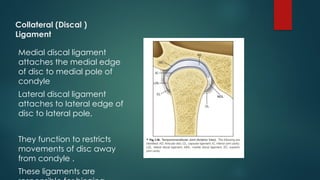
Collateral (Discal )
Ligament
Medialdiscal ligament
attaches the medial edge
of disc to medial pole of
condyle
Lateral discal ligament
attaches to lateral edge of
disc to lateral pole,
They function to restricts
movements of disc away
from condyle .
These ligaments are
30.
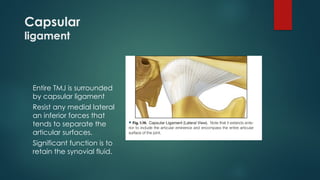
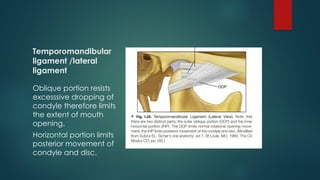
Capsular
ligament
Entire TMJ issurrounded
by capsular ligament
Resist any medial lateral
an inferior forces that
tends to separate the
articular surfaces.
Significant function is to
retain the synovial fluid.
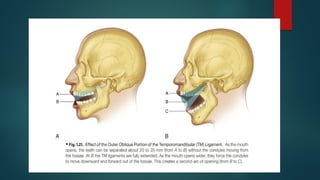
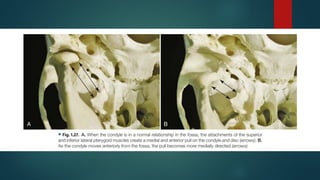
Lateral ligamentalso influences the normal opening movement of
condyle.
During initial phases of opening,condyle rotates around fixed point
until TMJ ligament becomes taut,after neck of condyle cannot
rotate further.If the mouth were to be open wider,condyle would
need to move downward and forward across the articular
eminence.
Condyle rotates open until the ,anterior teeth are 20 to 25 mm apart
,afterwards condyle shows translation to maximum mouth opening.
34.
The uniquefeature of TM Ligament,which limits rotational opening is
found only in humans.
BENEFIT- In erect postural position with a vertically placed vertebral
column continued rotational opening movement would cause
mandible to impinge on vital submandibular and retromandibular
structures of the neck.The outer oblique portion pf TM Ligament
functions to resist this impingement.
35.
Inner horizontalportion protects the retodiscal tissues from trauma
created by posterior displacement of condyle.
It also protects lateral pterygoid muscle from overlengthening.
In cases of extreme trauma to mandible, this portion of ligament
becomes tight and the neck of the condyle will seen to fracture
before retrodiscal tissues are severed or condyle enters the middle
cranial fossa.
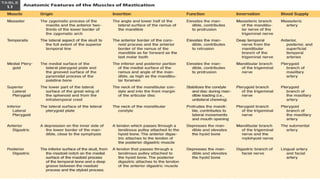
Muscles of mastication
Four pairs of muscles make up a group called the
muscles of mastication:
The masseter
The temporalis
The medial pterygoid
The lateral pterygoid
Diagastrics , sternocleidomastoid and posterior cervical
muscles enables controlled movement of mandible to
be performed.
39.
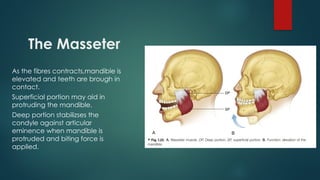
The Masseter
As thefibres contracts,mandible is
elevated and teeth are brough in
contact.
Superficial portion may aid in
protruding the mandible.
Deep portion stabilizses the
condyle against articular
eminence when mandible is
protruded and biting force is
applied.
40.
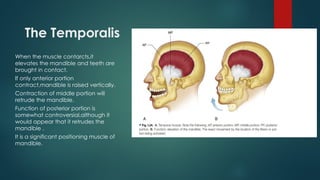
The Temporalis
When themuscle contarcts,it
elevates the mandible and teeth are
brought in contact.
If only anterior portion
contract,mandible is raised vertically.
Contraction of middle portion will
retrude the mandible.
Function of posterior portion is
somewhat controversial,although it
would appear that it retrudes the
mandible .
It is a significant positioning muscle of
mandible.
41.
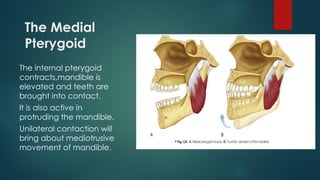
The Medial
Pterygoid
The internalpterygoid
contracts,mandible is
elevated and teeth are
brought into contact.
It is also active in
protruding the mandible.
Unilateral contaction will
bring about mediotrusive
movement of mandible.
42.
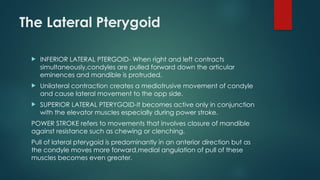
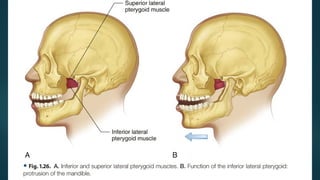
The Lateral Pterygoid
INFERIOR LATERAL PTERGOID- When right and left contracts
simultaneously,condyles are pulled forward down the articular
eminences and mandible is protruded.
Unilateral contraction creates a mediotrusive movement of condyle
and cause lateral movement to the opp side.
SUPERIOR LATERAL PTERYGOID-It becomes active only in conjunction
with the elevator muscles especially during power stroke.
POWER STROKE refers to movements that involves closure of mandible
against resistance such as chewing or clenching.
Pull of lateral pterygoid is predominantly in an anterior direction but as
the condyle moves more forward,medial angulation of pull of these
muscles becomes even greater.
45.
Biomechanics of TMJ–its structure and function
can be divide into two distinct system
One joint system
It involves tissues that surround
inferior synovial cavity that is
condyle and articular disc.
Since disc is tightly bound to
condyle by discal ligaments ;only
rotational movement of the disc
around condyle is possible.
This condyle disc complex is
responsible for rotational
movement in TMJ.
Second joint system
It consists of condyle disc
complx against surface of
mandibular fossa.
Since disc is not tightly attached
to fossa,free sliding movement is
possible in superior cavity
referred to as translation when
the mandible is moved forward.
47.
Joint stability
Thearticular surface of TMJ have no structural attachment ,yet
contact must be maintained constantly for joint stability which is
maintained by constant activity of muscle pull.
Even in resting state ,muscle are tonus.When activity
increases,condyle is increasingly forced against disc and disc
against fossa resulting in increase in interarticular pressure of these
joint structures.In absence of interarticular pressure,articular surfaces
will separate and joint will technically dislocate.
Width of articular disc space varies with interarticular pressure.When
pressure is low ,as in closed rest position,disc space widens tightly.
When pressure is high as in clenching,disc space narrows.
48.
The contourand the movement of disc permits constant contact of
articular surfaces of joint necessary for joint stability.
When pressure increases,condyle seat on thinner intermediate zone
When pressure is low and disc space is widened ,thicker portion of disc
is rotated to fill the space.
49.
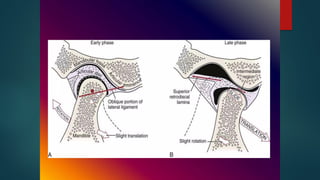
When themouth is closed,the elastic traction on the disc is minimal
to none.
But during mouth opening,condyle is pulled forward down the
articular eminence,superior retrodiscal lamina becomes increasingly
stretched creating increased forces to retract the disc and only
structure capable of retracting the disc.
The interarticular pressure and morphology of disc prevents the disc
from being overretracted.In other words,as the mandible moves
into fully position and during return,retraction force hold the disc
rotated as far posteriorly on the condyle as width of articular disc will
permit.
50.
In thisway during translation,the interaticular pressure and
morphology of disc maintains the condyle on intermediate zone
and disc is forced to translate forward with condyle.
Only when the morphology is altered does the ligamenteous
attachment of disc affect joint function.
When this occurs,biomechanics of the joint isaltered and
dysfunctional signs begin.
51.
REFERENCES
Jeffrey P OkesonManagement of
Temporomandibular disorders and
Occlusion
Orban’s Oral Histology &
Embryology

























![Temporomandibular joint [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/temporomandibularjointautosaved-230521065437-1cbd4148-thumbnail.jpg?width=640&height=640&fit=bounds)




























