Downloaded 122 times








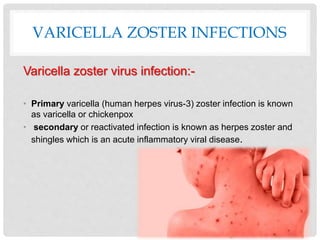
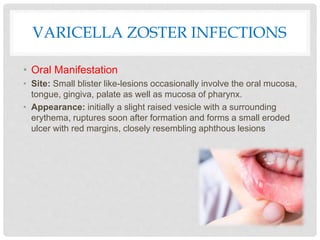
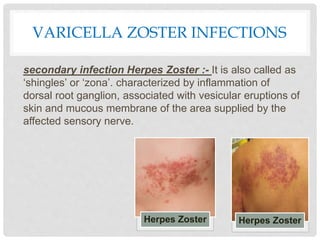
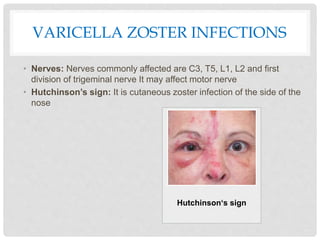
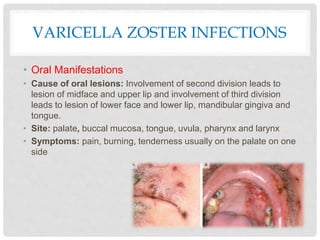

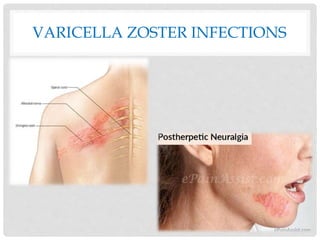

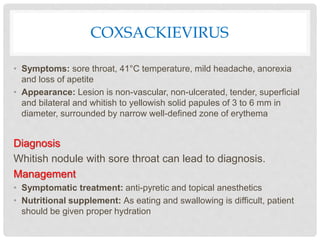
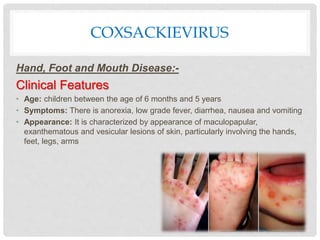
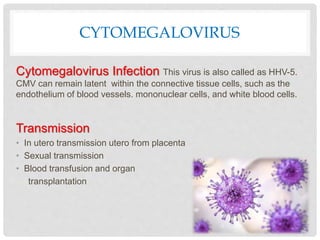




The document provides an extensive overview of viral infections affecting the oral cavity, detailing the characteristics, symptoms, diagnosis, and management of various viruses including herpes simplex virus, varicella zoster virus, coxsackievirus, cytomegalovirus, and measles virus. It describes the clinical manifestations, transmission methods, and treatment options for each virus. Additionally, the document highlights the potential complications arising from these infections, particularly in immunocompromised patients.










![Fungal infections of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/fungalinfectionsofskincompatibilitymode-130321223403-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
























































