- Status epilepticus has a worldwide incidence of 3.8 to 38 per 100,000 people per year, with peaks in children and the elderly. Around 31-44% of cases are refractory to initial treatment.
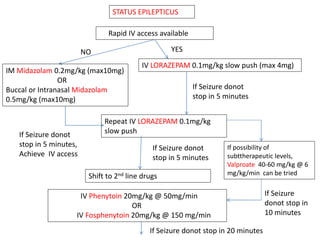
- Initial treatment involves benzodiazepines like lorazepam or diazepam. If seizures continue, second-line drugs like phenytoin, fosphenytoin, or valproate are used.
- Refractory status epilepticus is defined as failure to control seizures with benzodiazepines and other antiepileptics. It requires general anesthesia with drugs like propofol, thiopental, or midazolam along with
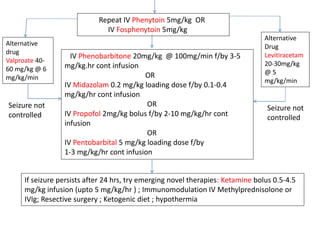






















































![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)

































