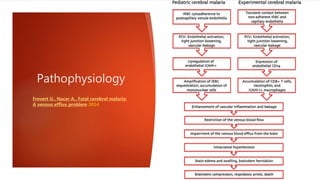
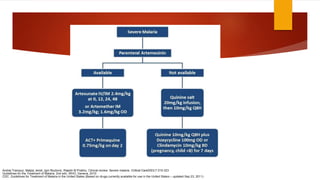
Cerebral malaria is a serious neurological complication caused by Plasmodium falciparum infection that can lead to coma and death. It accounts for approximately 20% of adult and 15% of childhood malaria deaths globally each year. The document discusses the epidemiology, transmission, clinical manifestations including retinopathy-specific signs, diagnosis, treatment and management of cerebral malaria. Pathophysiological mechanisms contributing to cerebral malaria are still being investigated.