Download to read offline
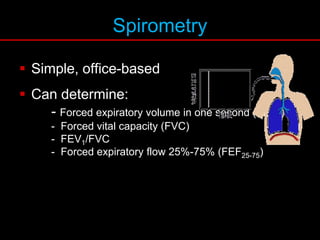
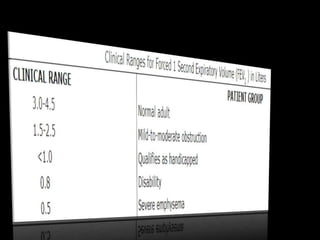
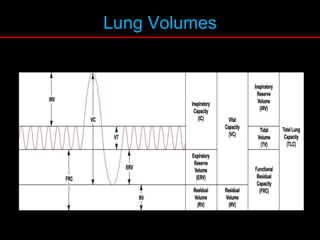
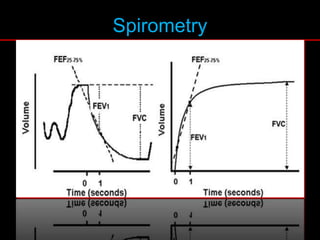
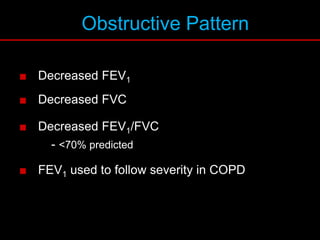
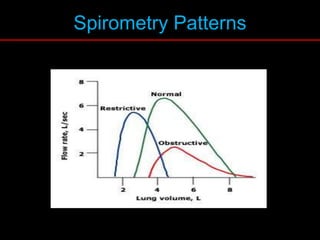
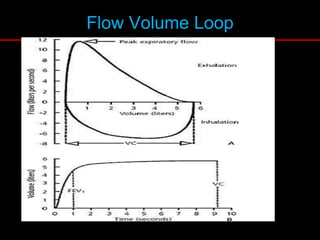
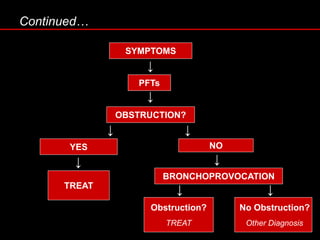
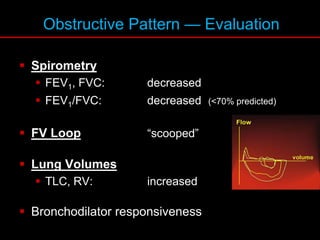
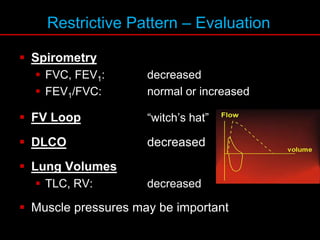
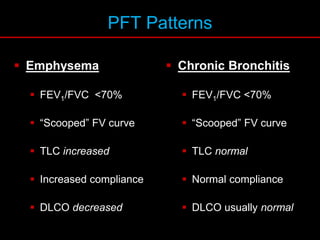


Pulmonary function tests (PFTs) measure how well the lungs work. Key PFT measurements include forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and their ratio (FEV1/FVC). PFTs can detect obstructive or restrictive lung patterns. In an obstructive pattern, FEV1 and FVC are reduced with a reduced FEV1/FVC ratio. A restrictive pattern shows reduced FEV1 and FVC but a normal or increased FEV1/FVC ratio. PFTs are used to diagnose and monitor lung diseases, evaluate patients for surgery, and guide treatment.













































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









