Downloaded 111 times






![FALLS EFFICACY SCALE
Rate level of confidence in doing each of the activities without
falling (0 = not at all, 10 = completely confident). Total score is
sum of 10 individual scores (range: 0 [low self-efficacy] to 100
[high self- efficacy]).
1. Cleaning house
2. Getting dressed and undressed
3. Preparing simple meals
4. Taking a bath or shower
5. Simple shopping
6. Getting in and out of car
7. Going up and down stairs
8. Walking around neighborhood
9. Reaching into cabinets and closets
10. Hurrying to answer the phone](https://image.slidesharecdn.com/assessmentofbalance-190721120816/75/Assessment-of-balance-11-2048.jpg)



![Modified version of the Functional Reach test
(modified Functional Reach Test [MFRT]) has been
developed. The test involves measuring unsupported
reaching in the forward and lateral direction in the
seated position.](https://image.slidesharecdn.com/assessmentofbalance-190721120816/75/Assessment-of-balance-15-2048.jpg)






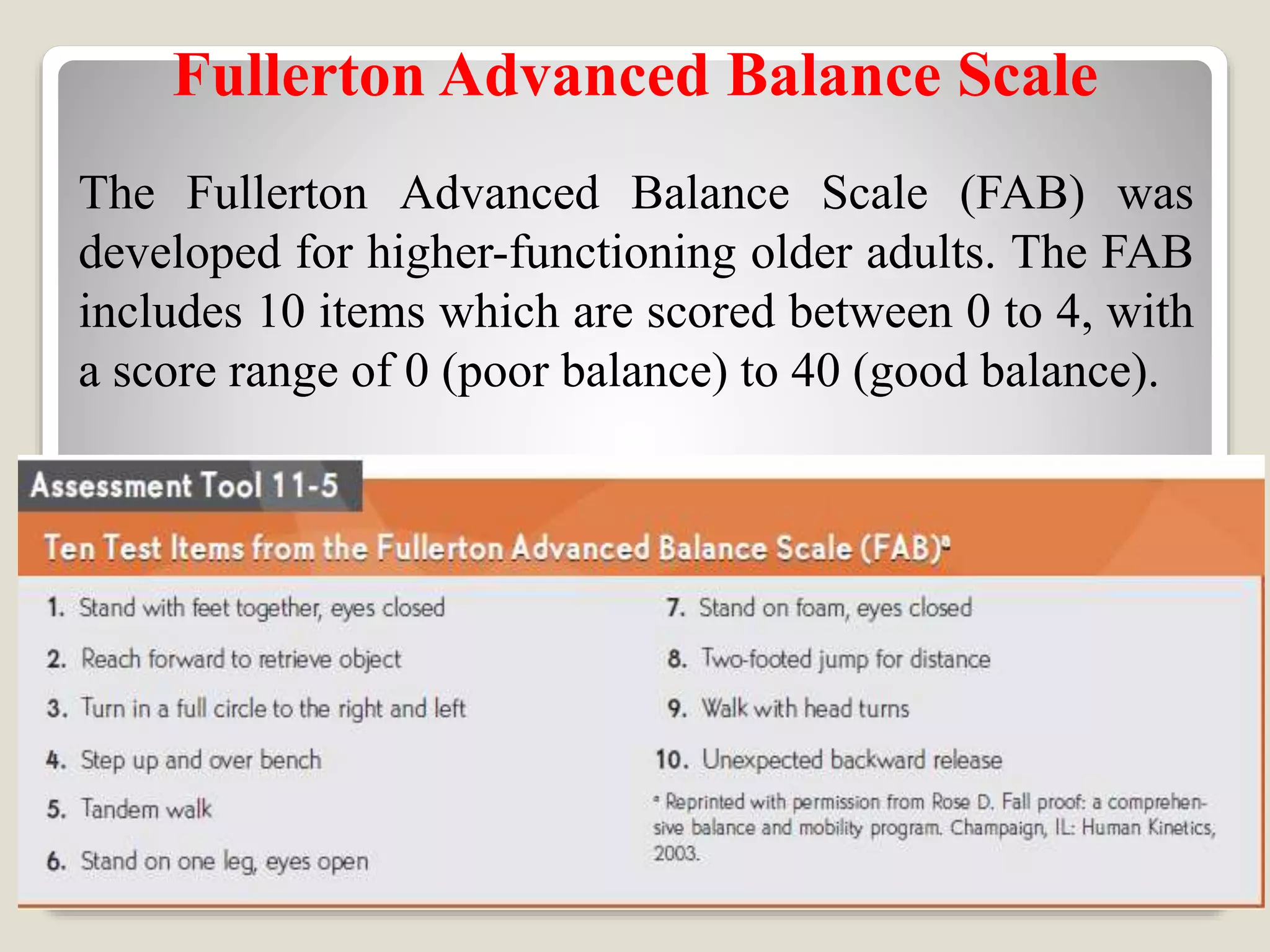


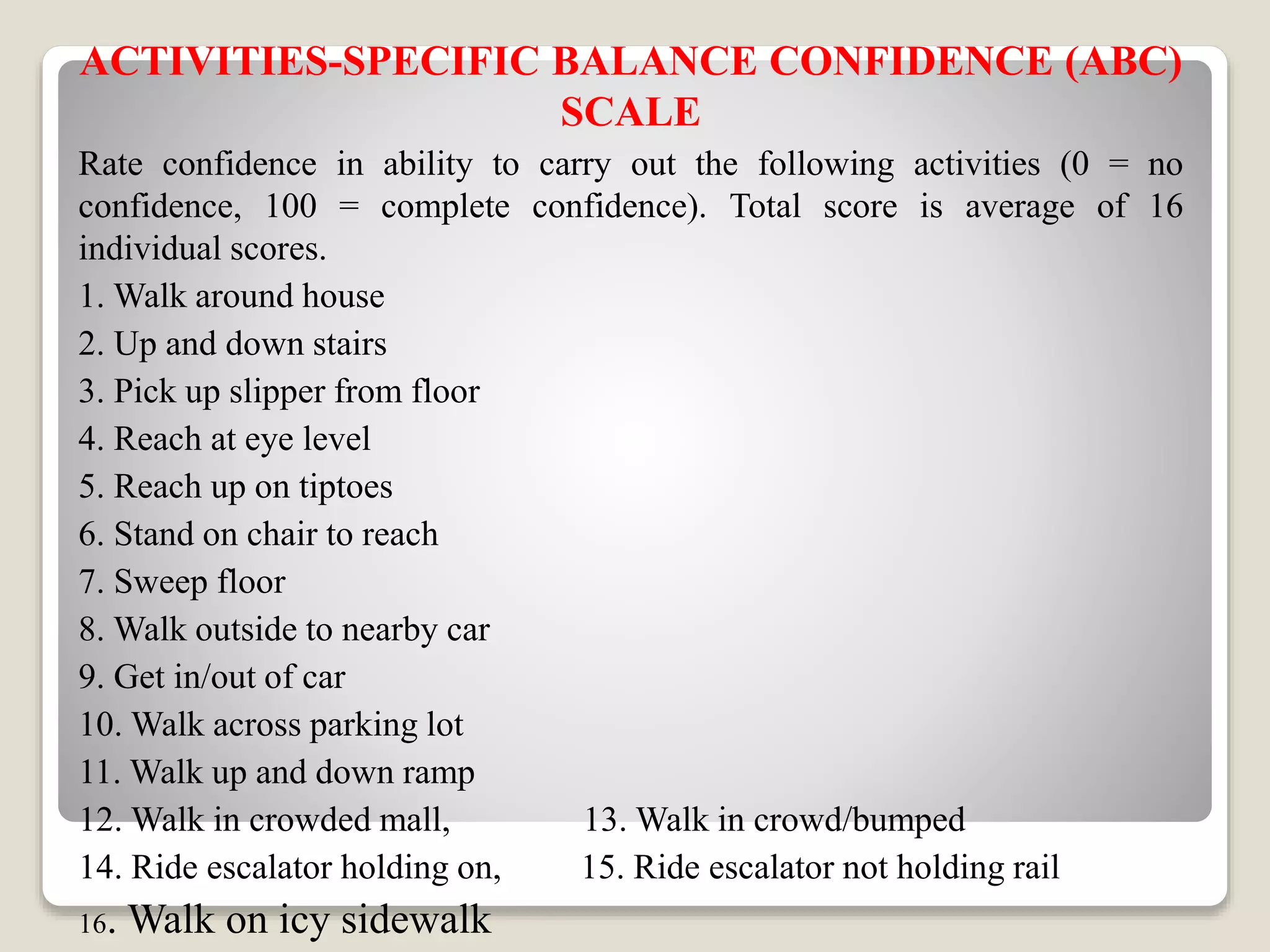
The document provides a comprehensive overview of balance assessment tools and methods used to evaluate postural control and fall risk, particularly in older adults. It details various tests such as the Activities-Specific Balance Confidence scale, Timed Up and Go test, and the Berg Balance Scale, along with their scoring systems and applications. Emphasis is placed on safety during examinations and the functional implications of balance assessments.



































































