Download as PDF, PPTX
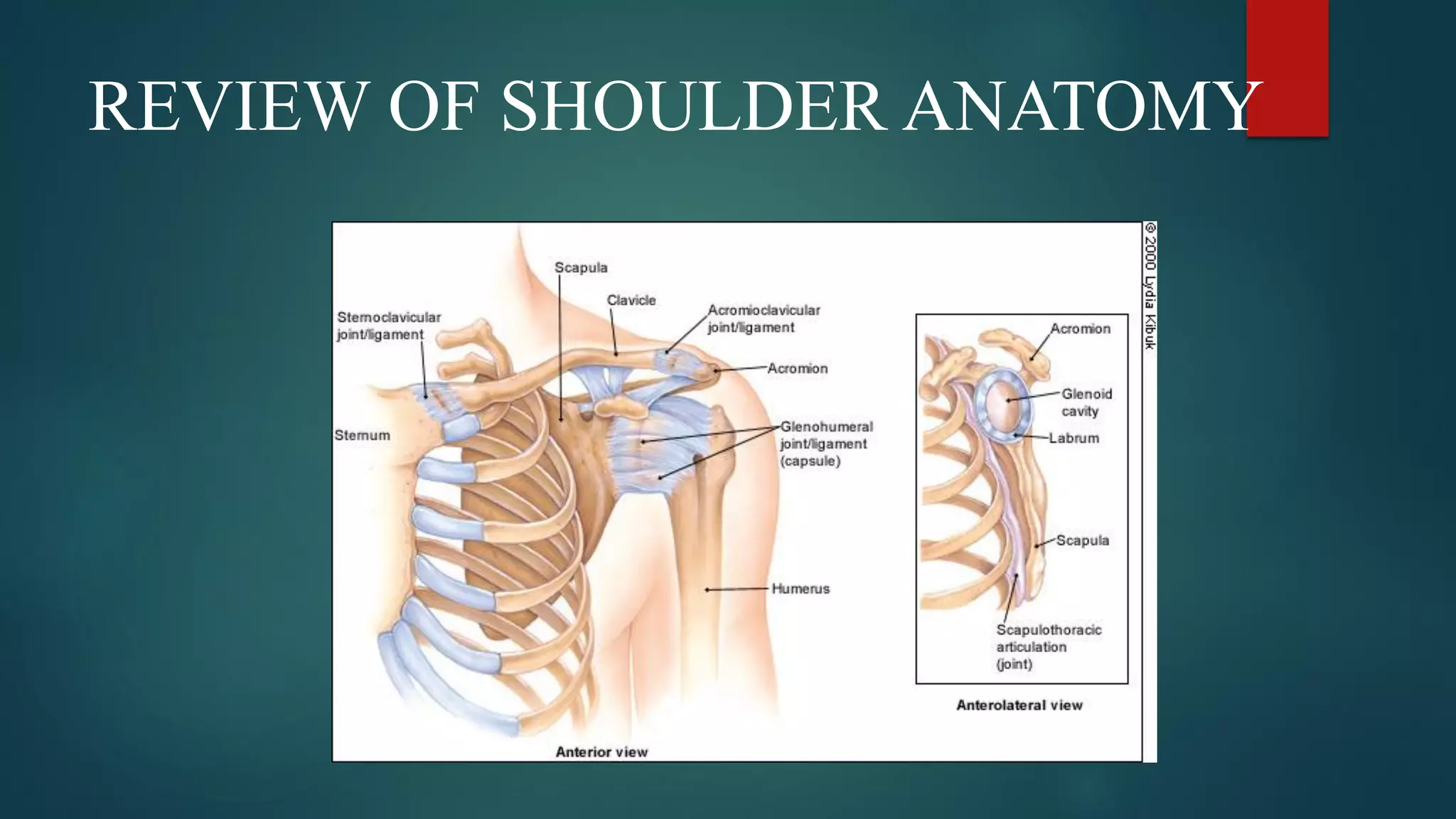
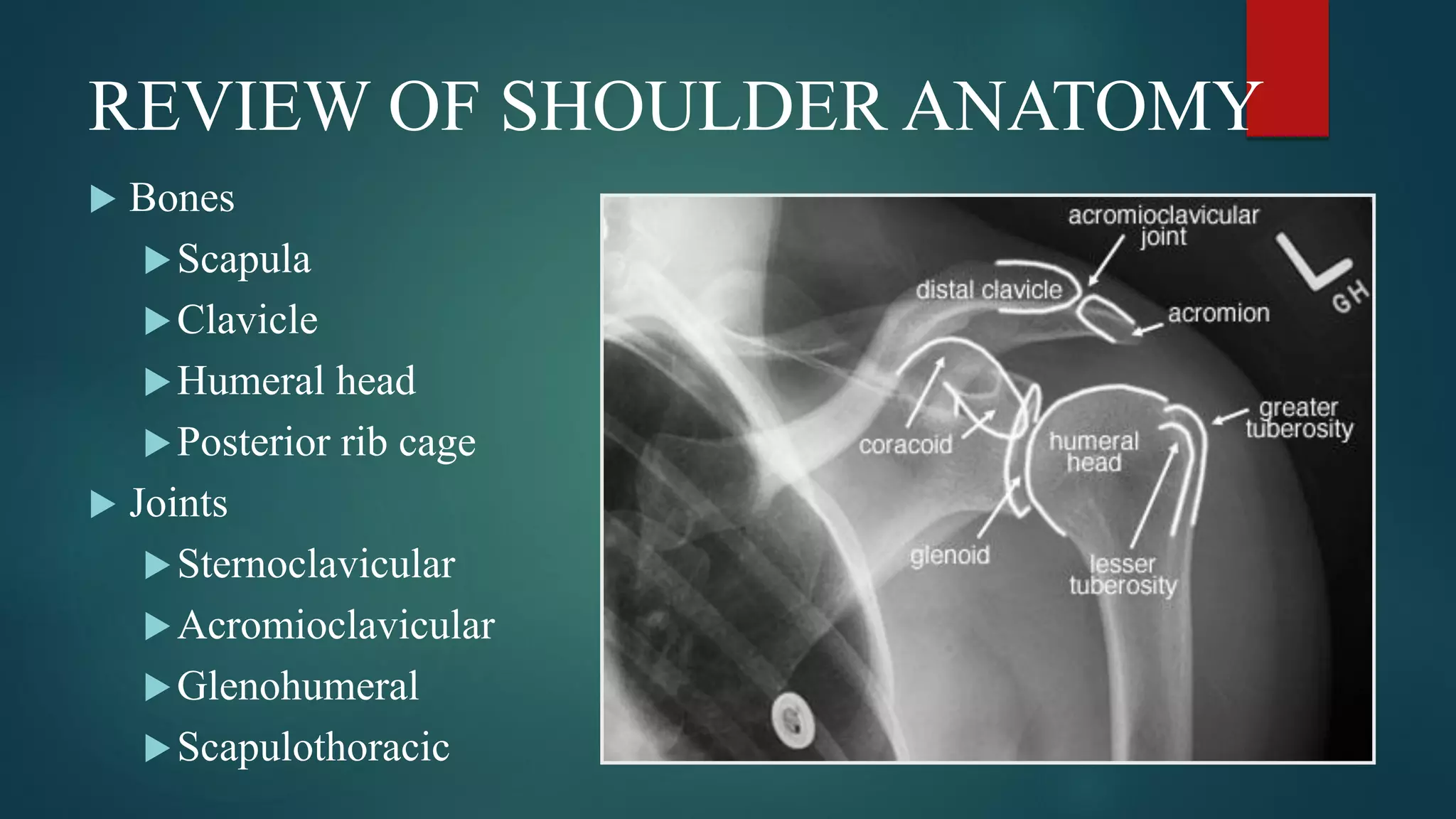
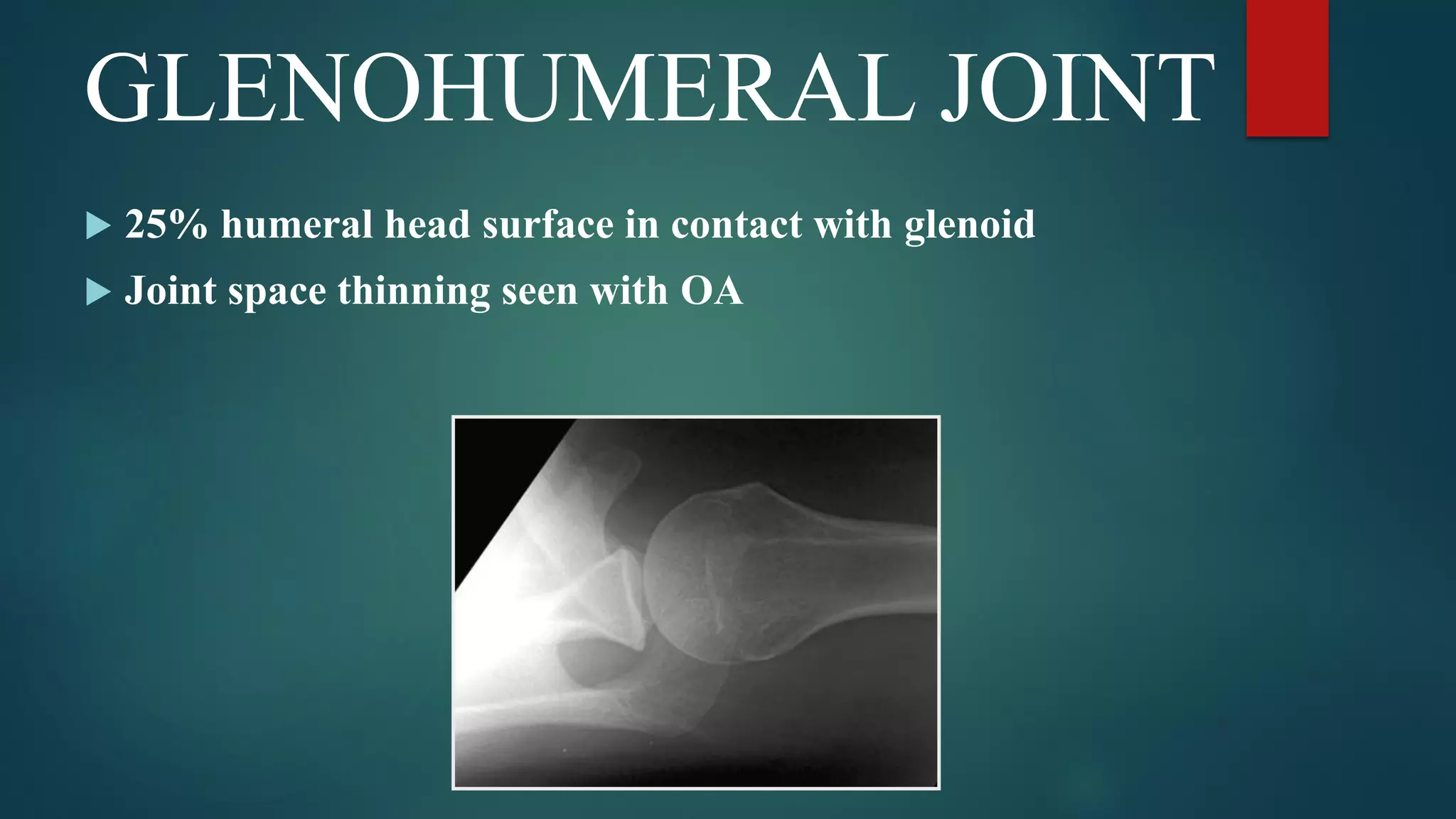
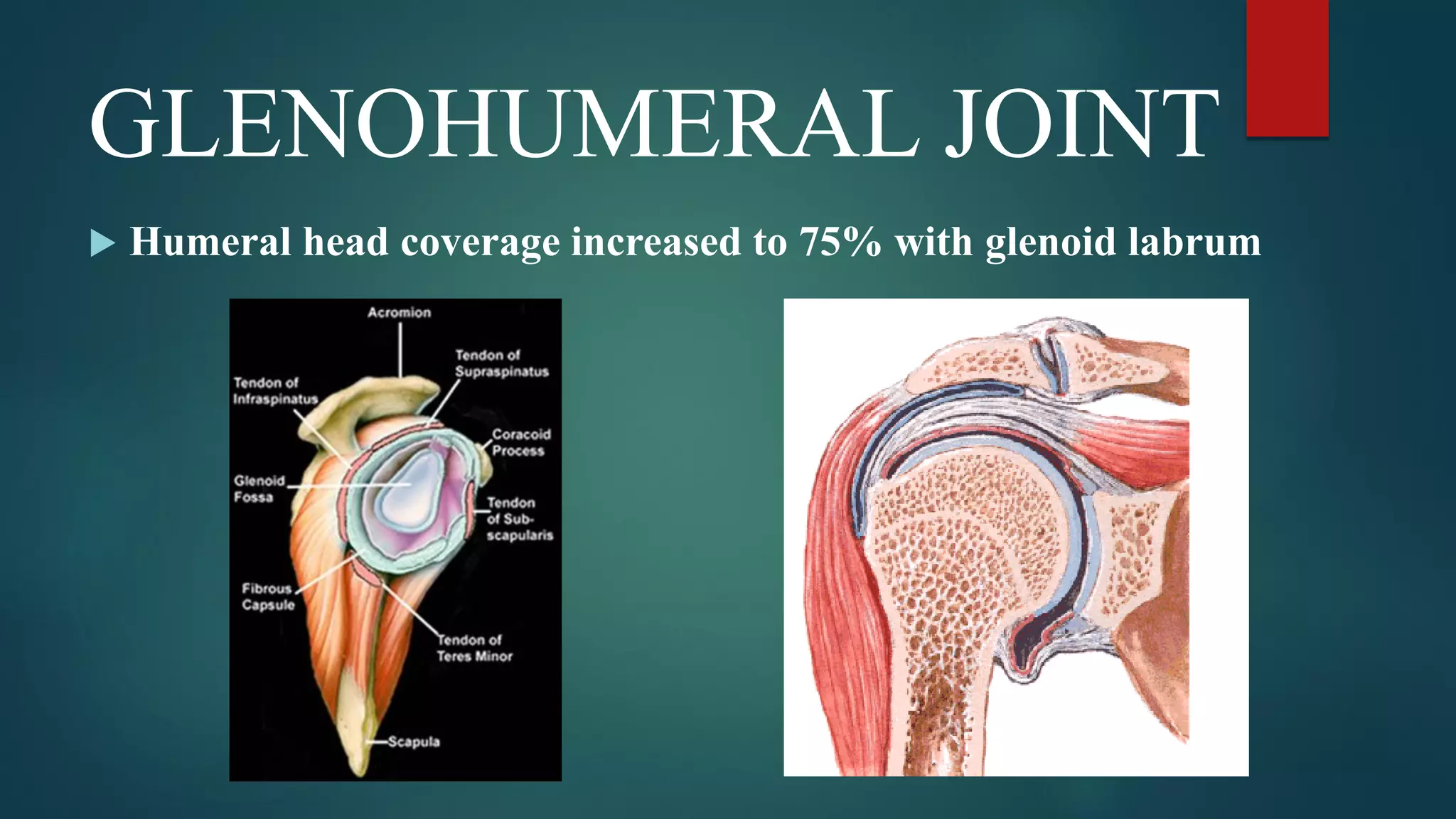
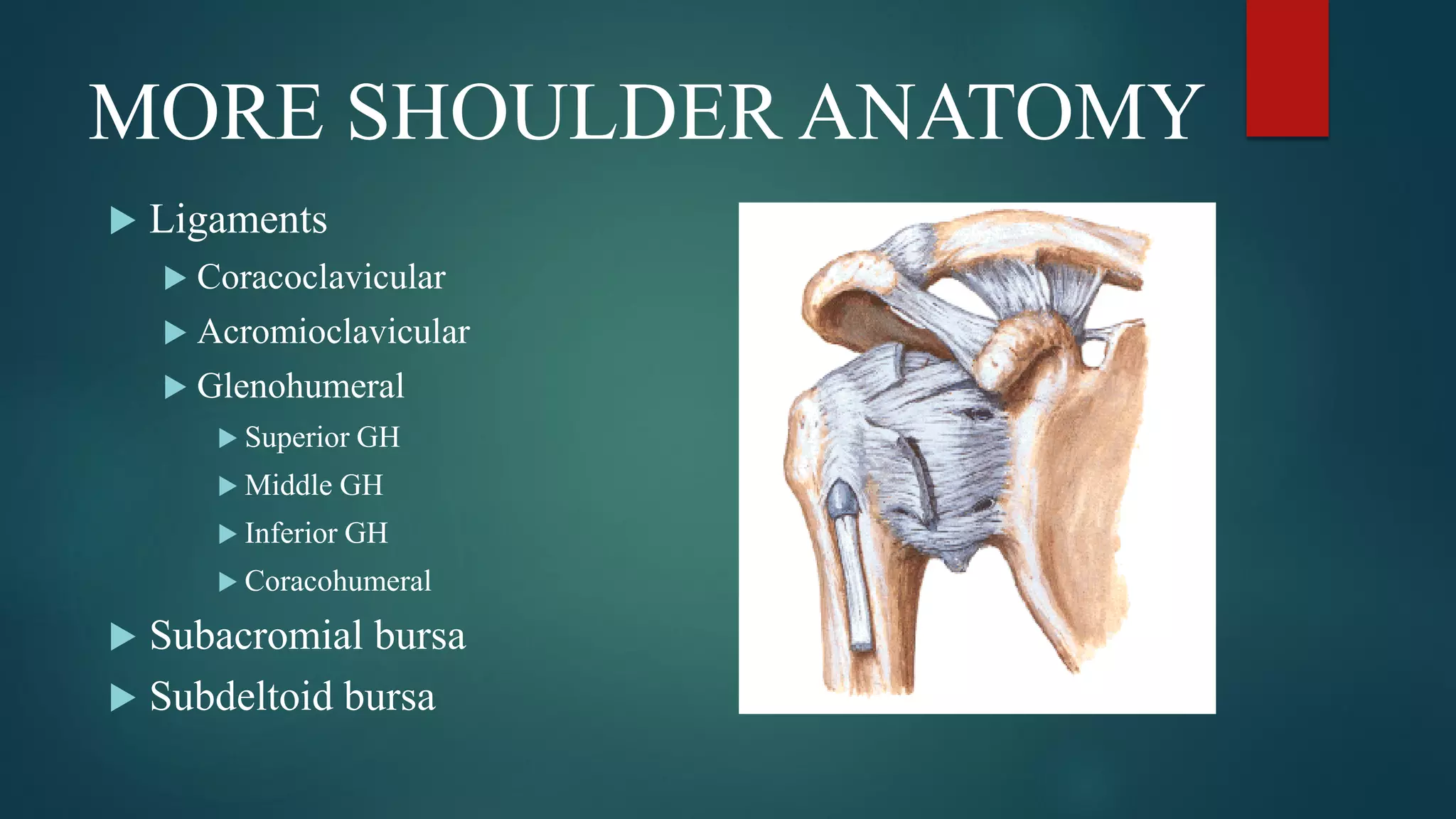
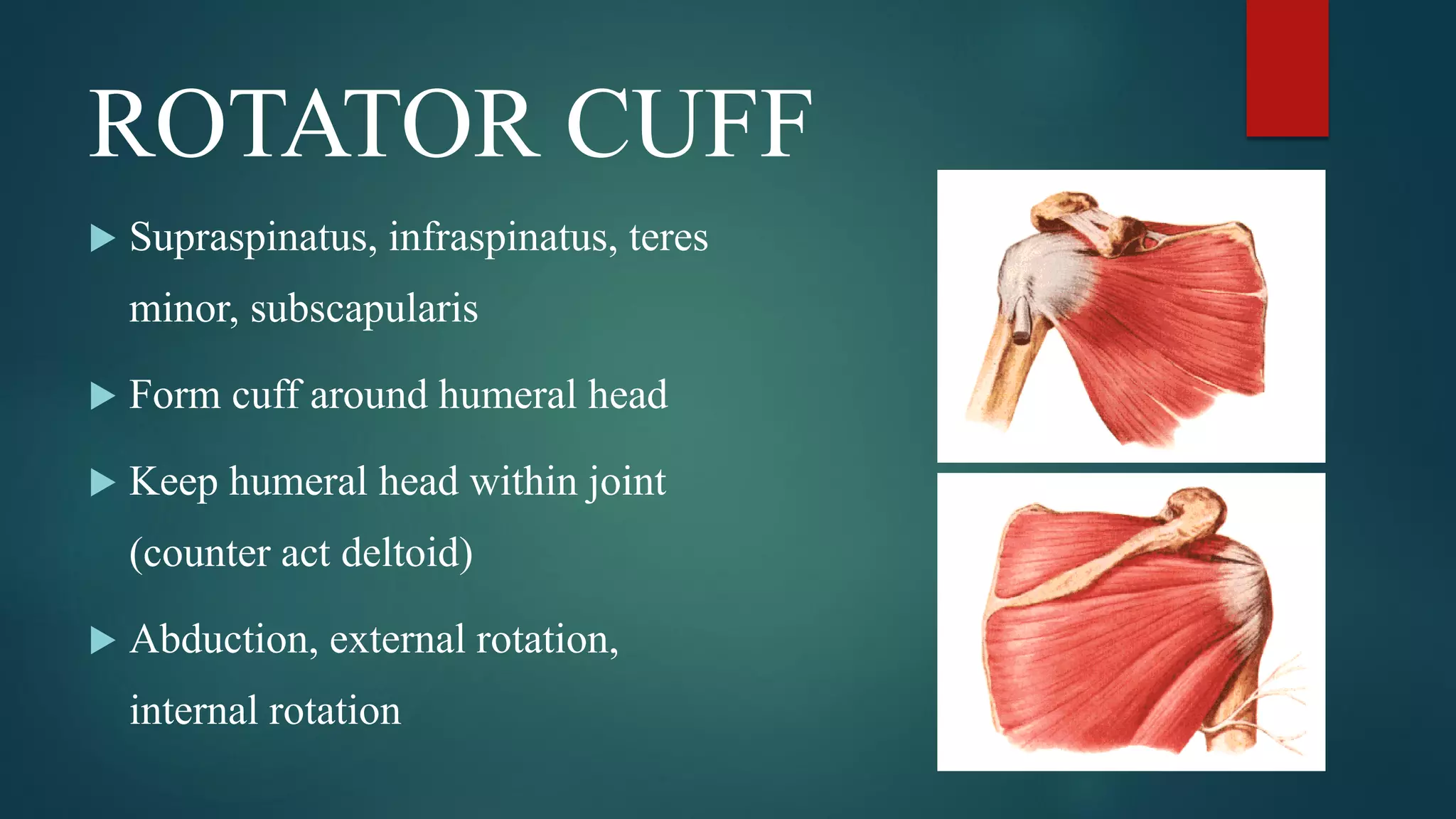

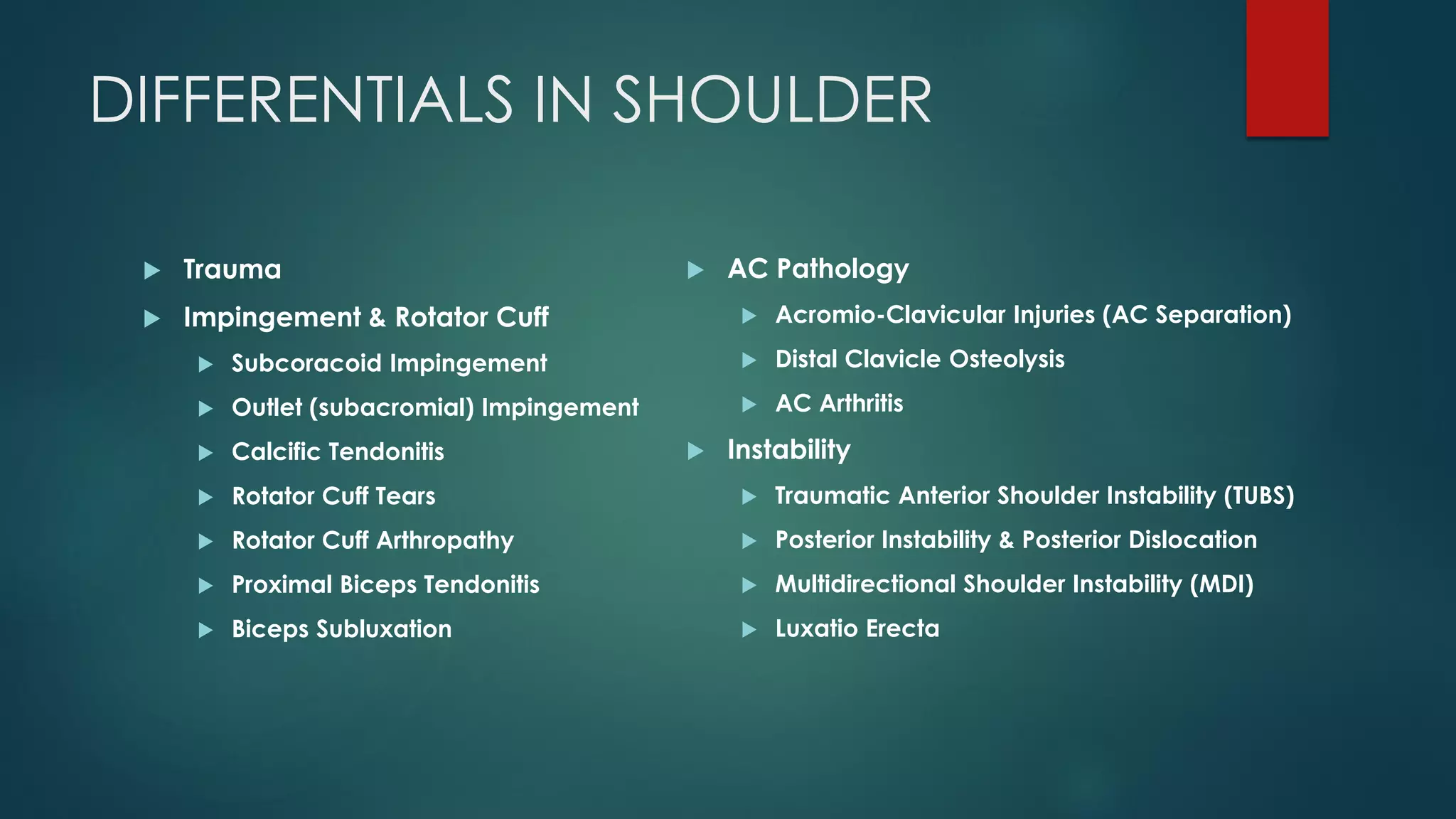
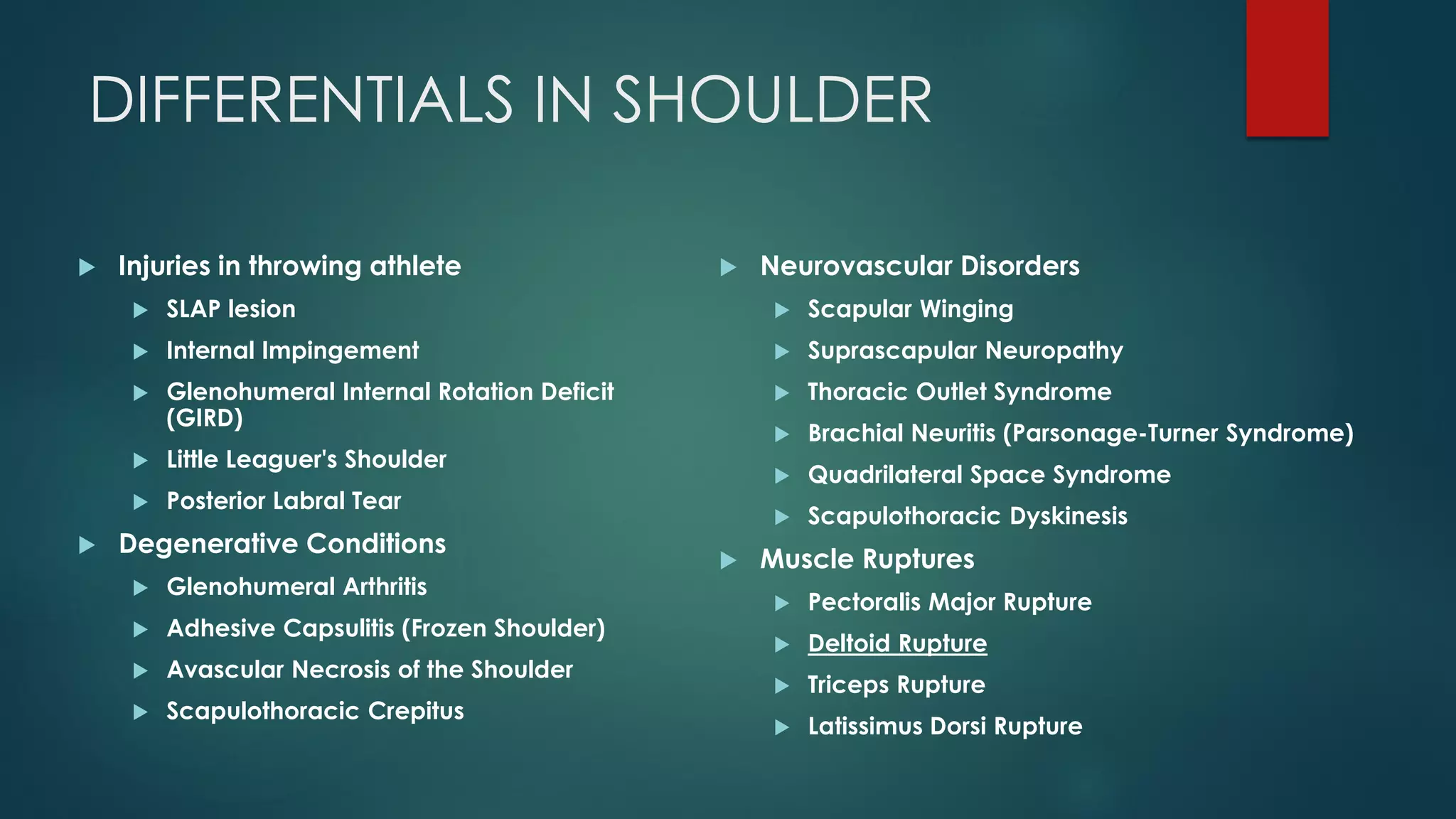
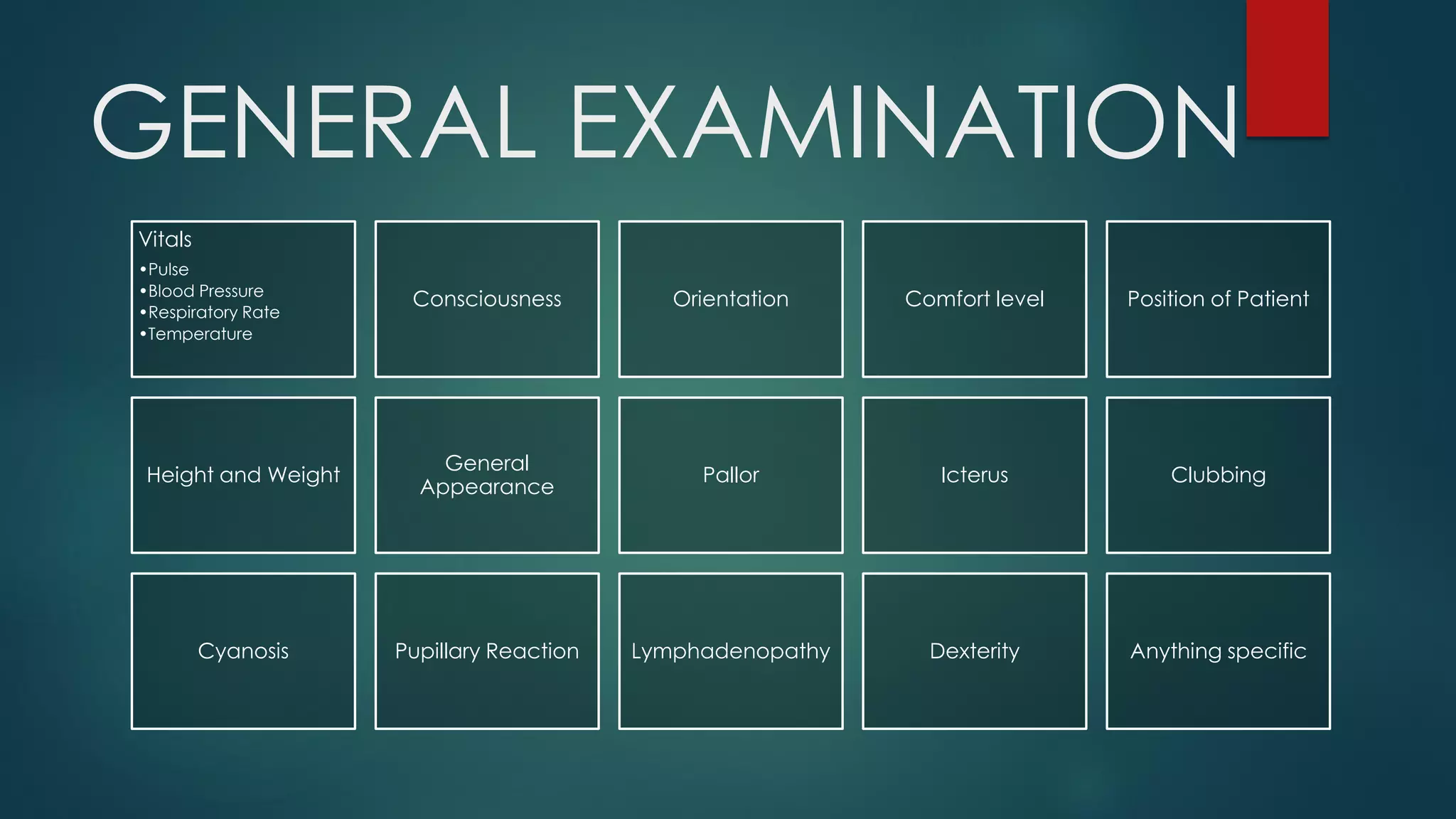
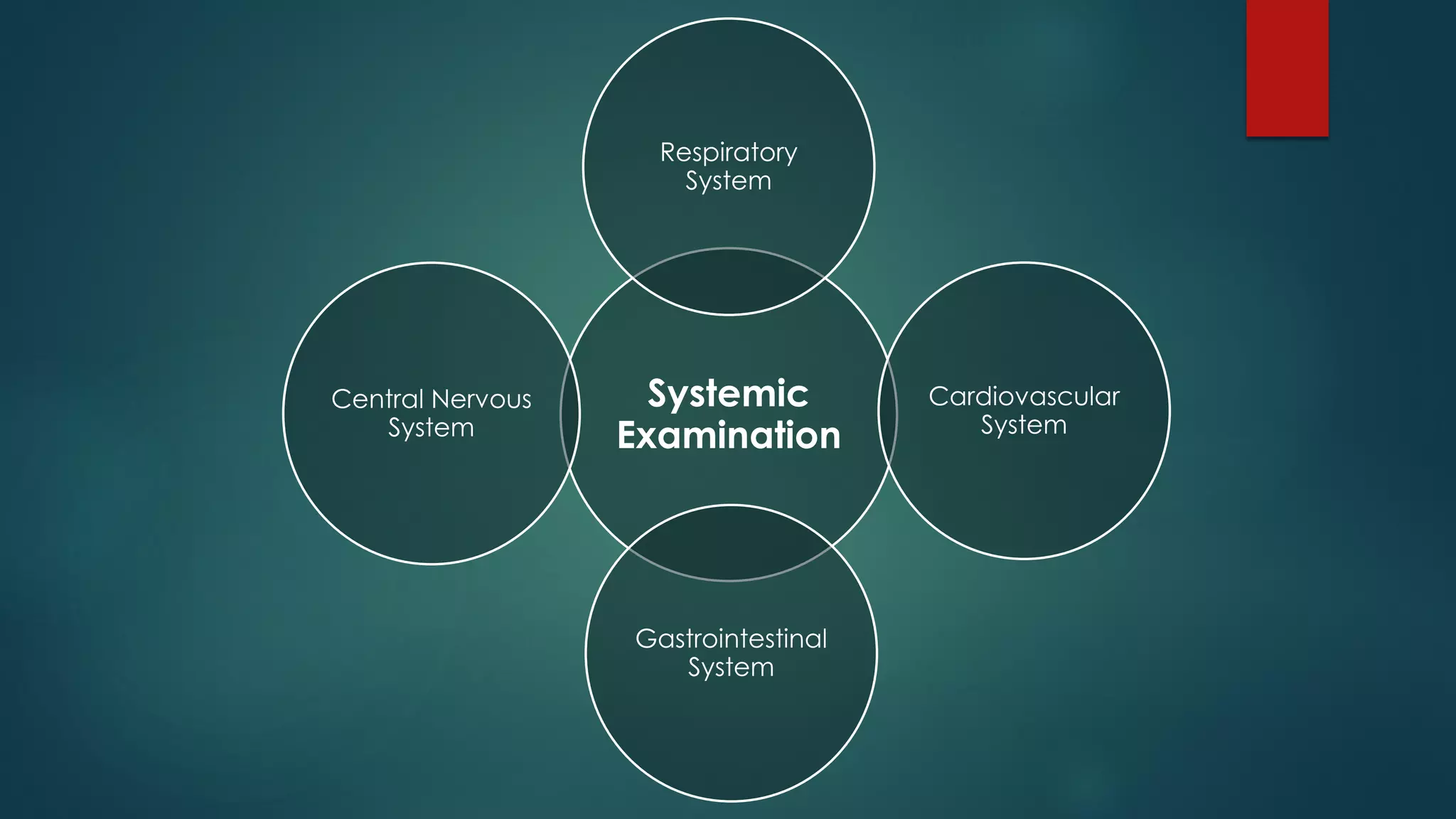
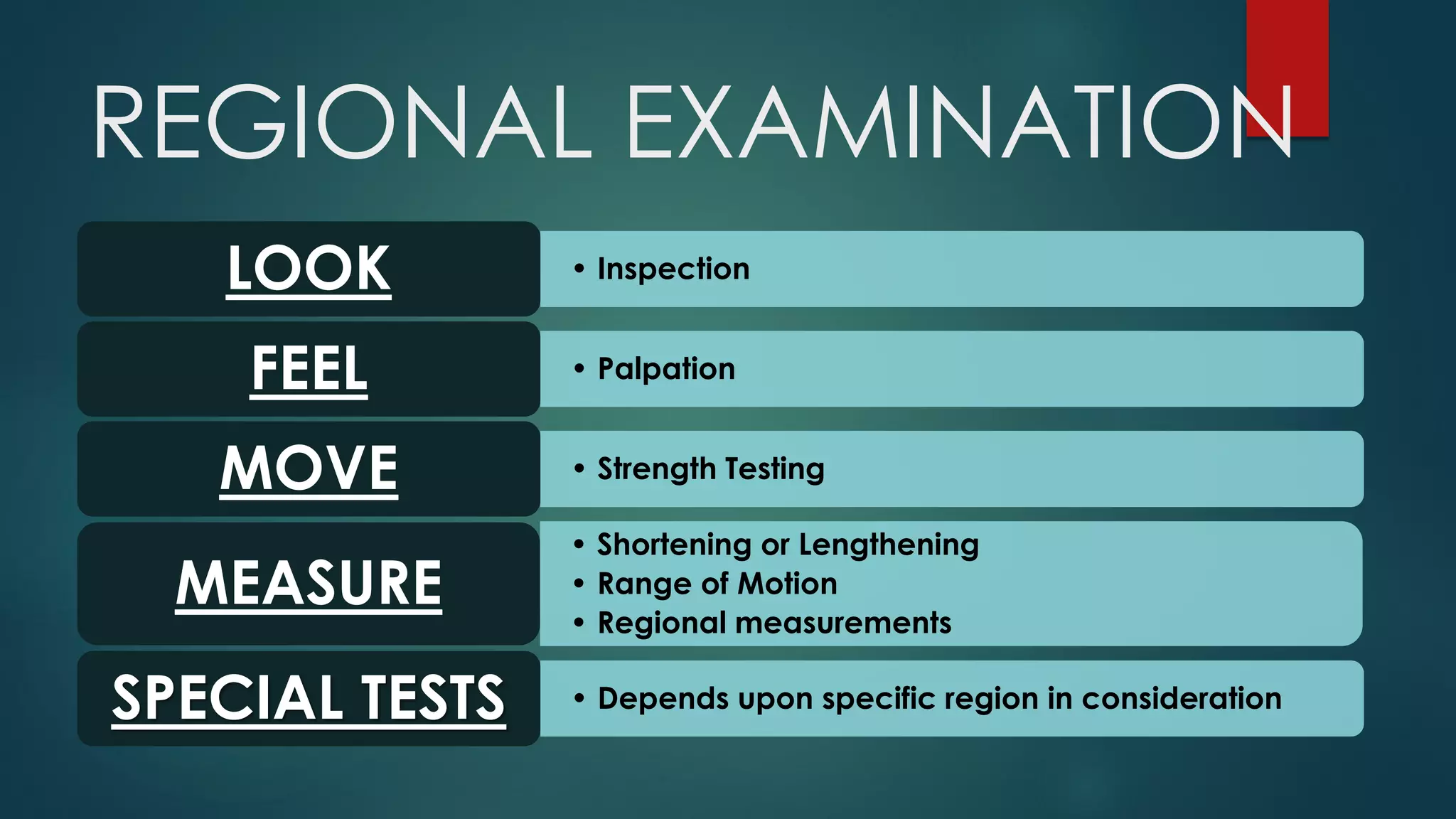
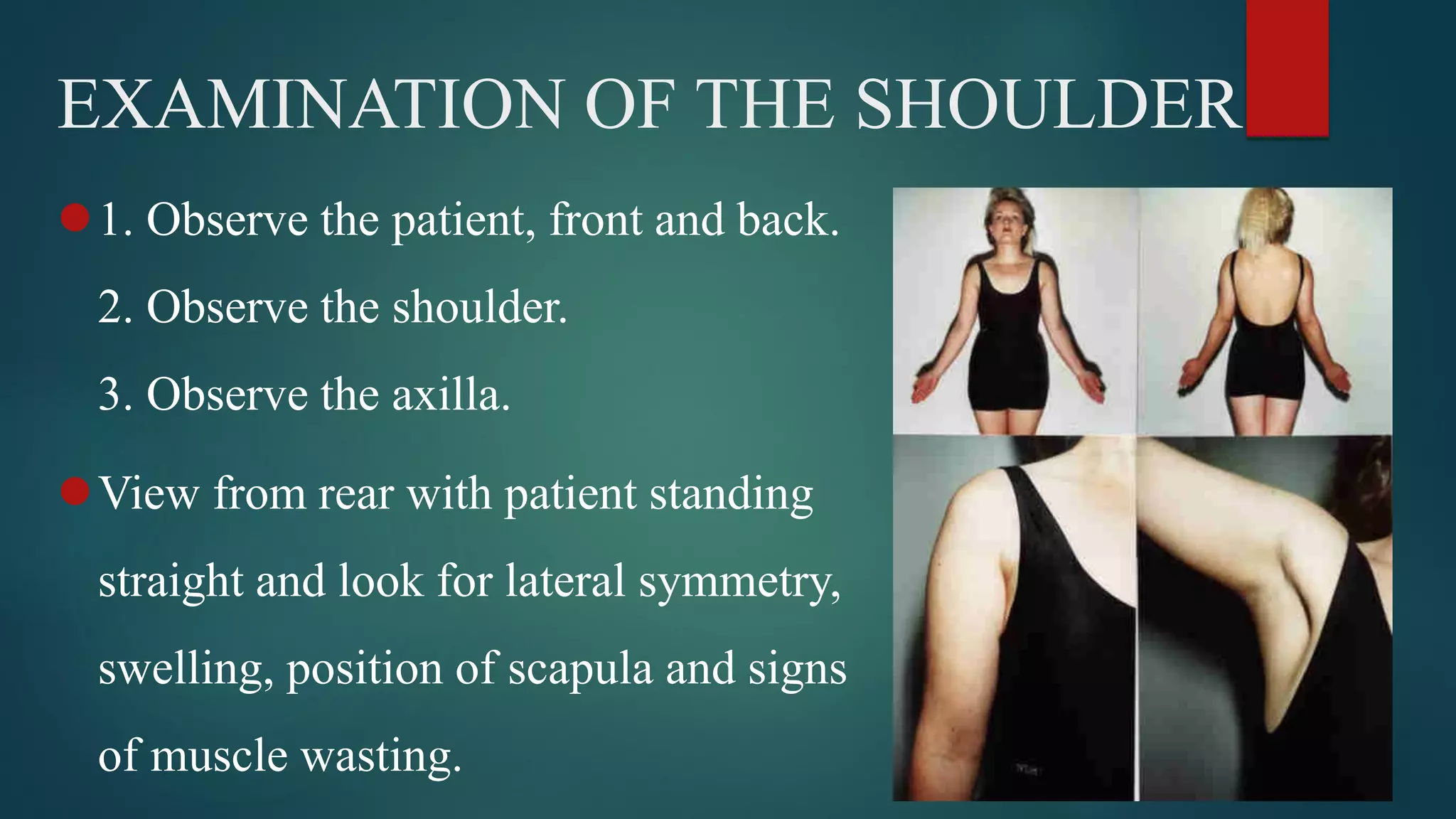
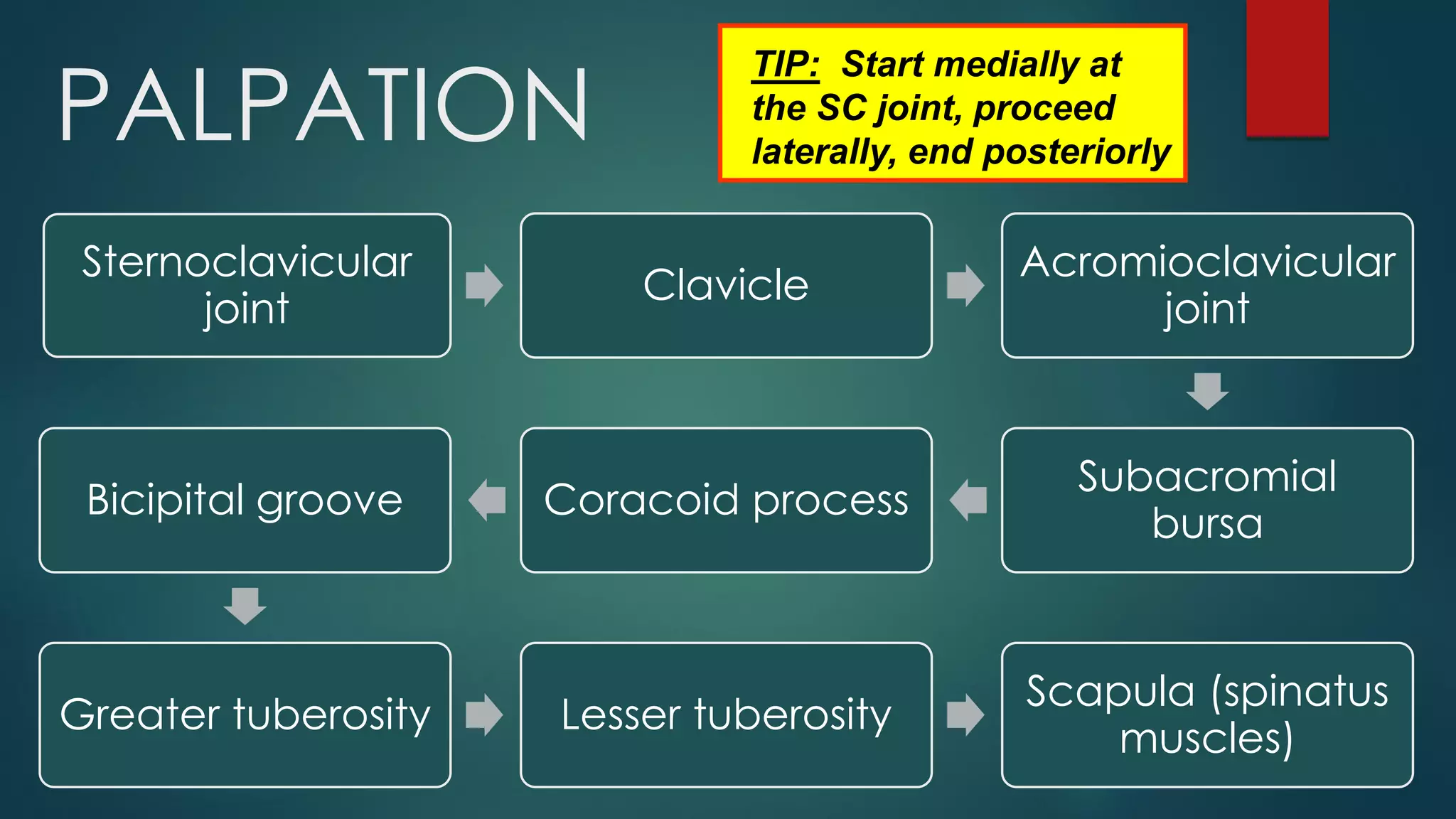
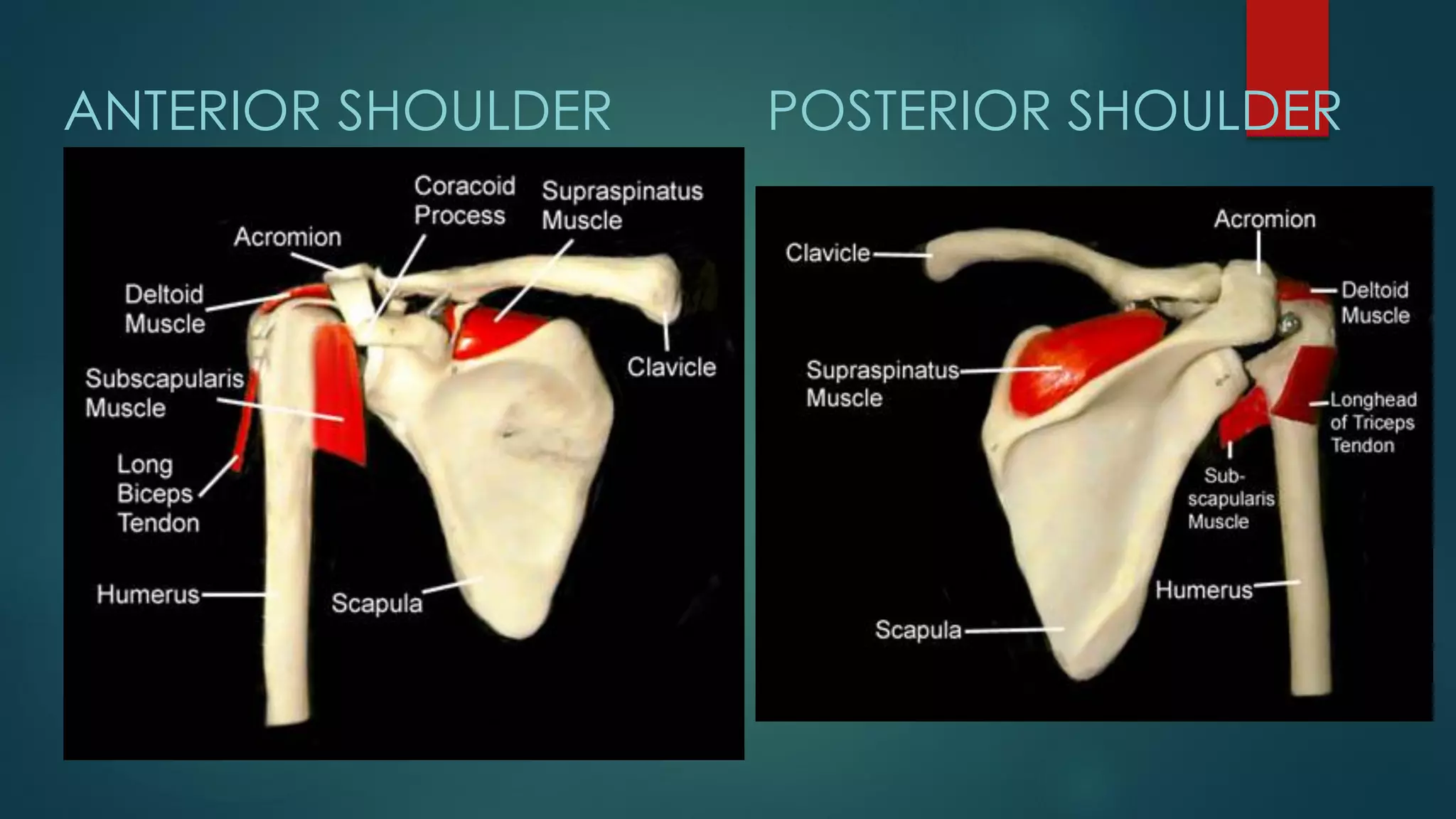
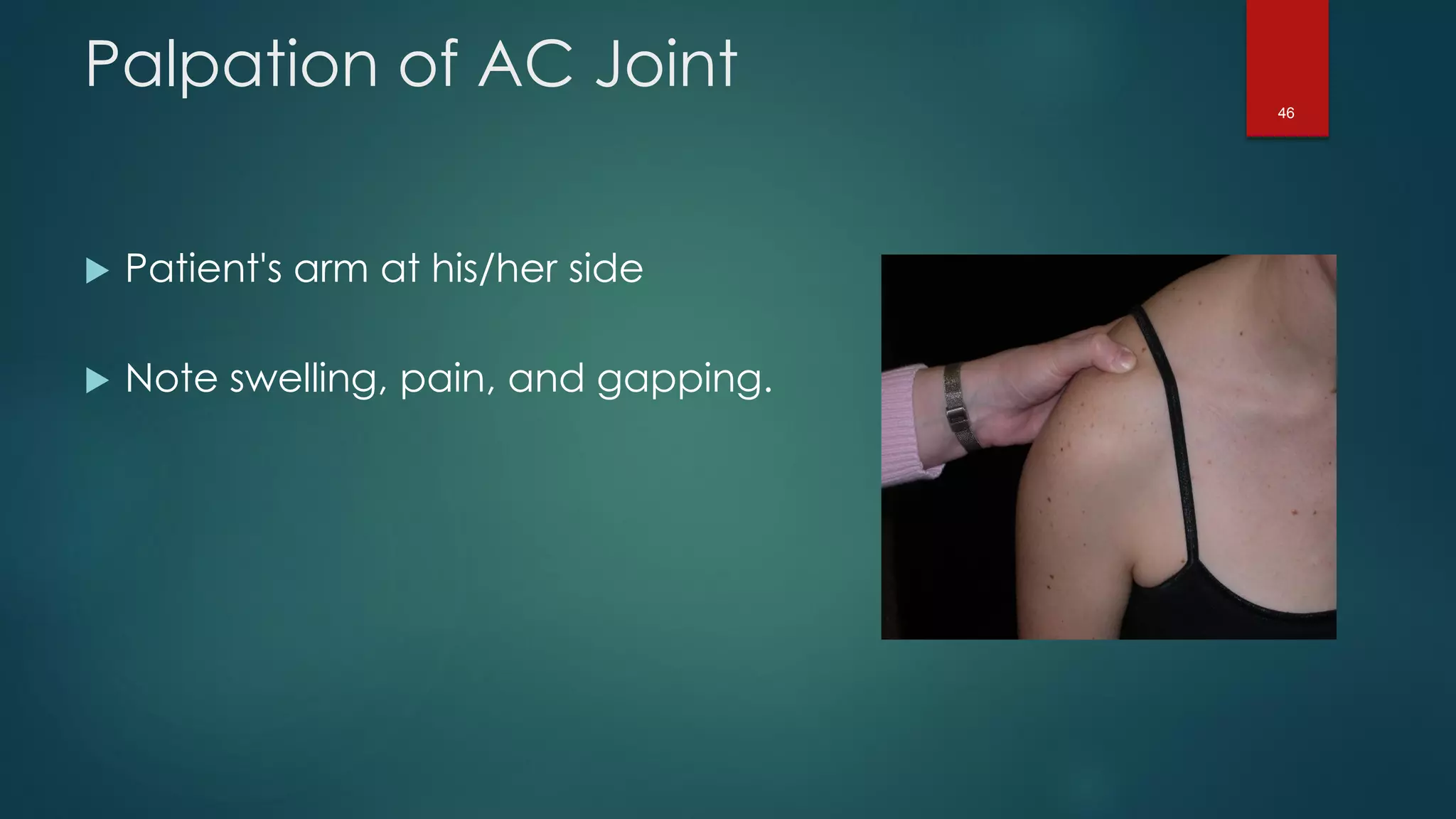
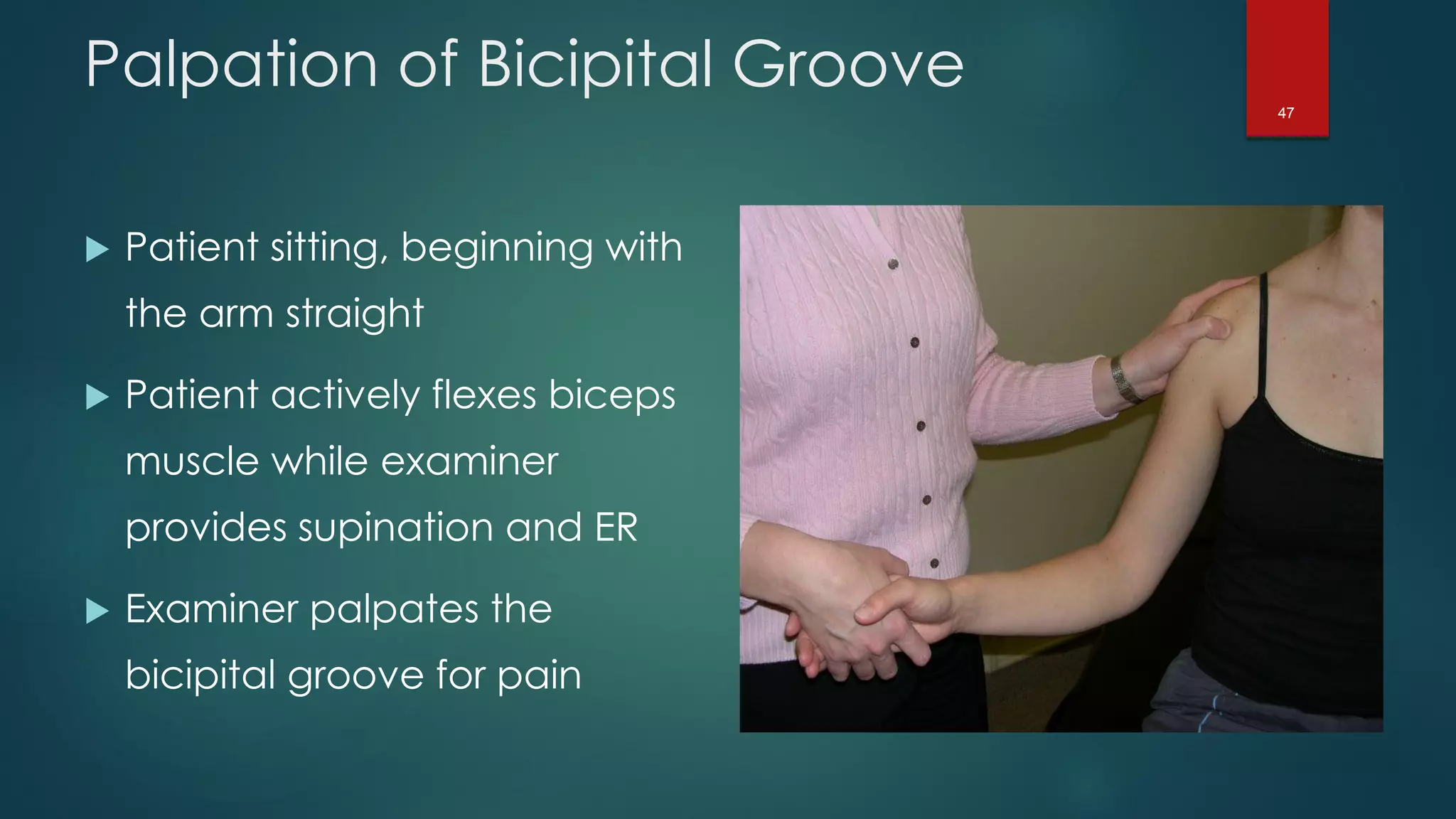
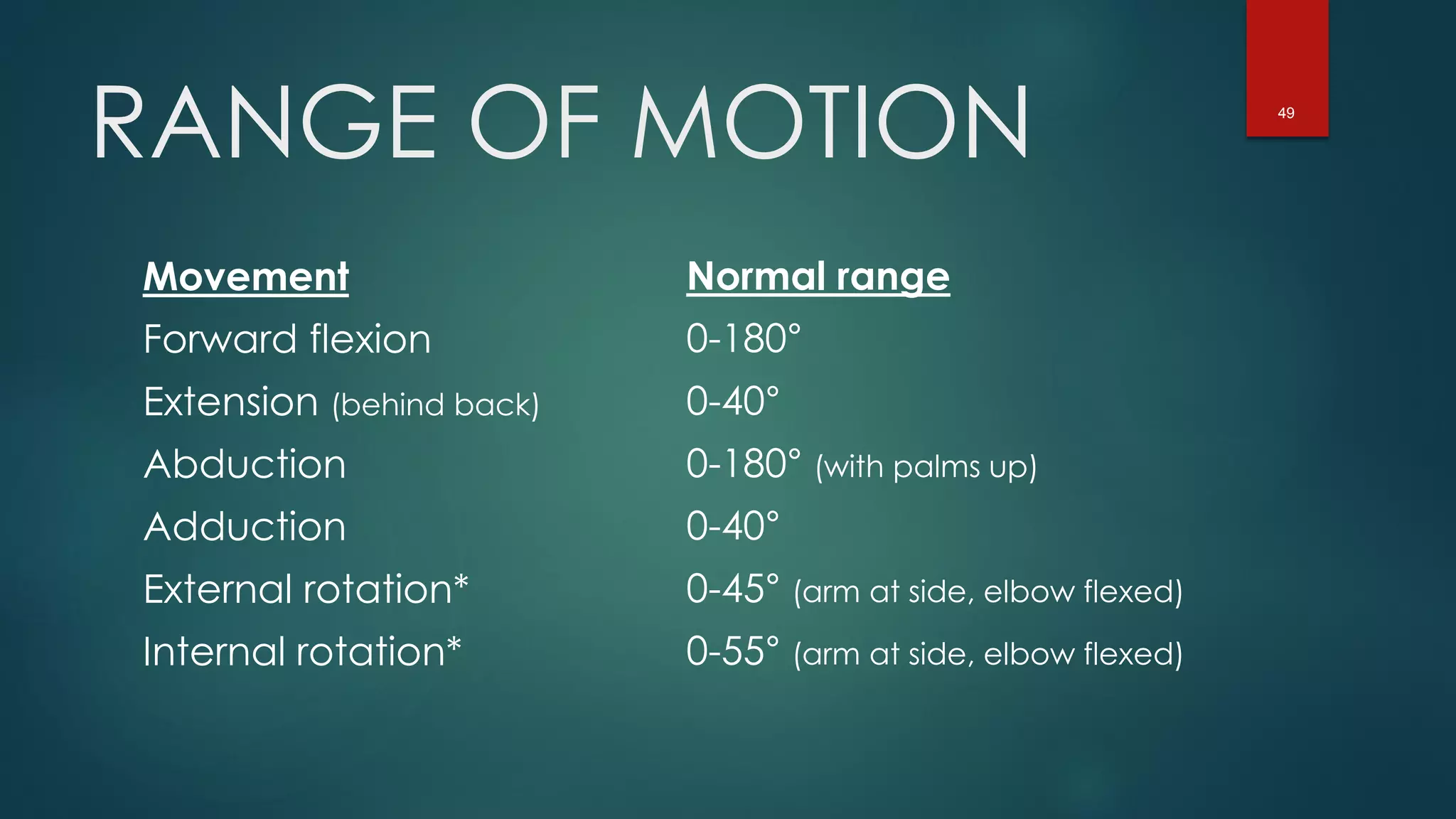
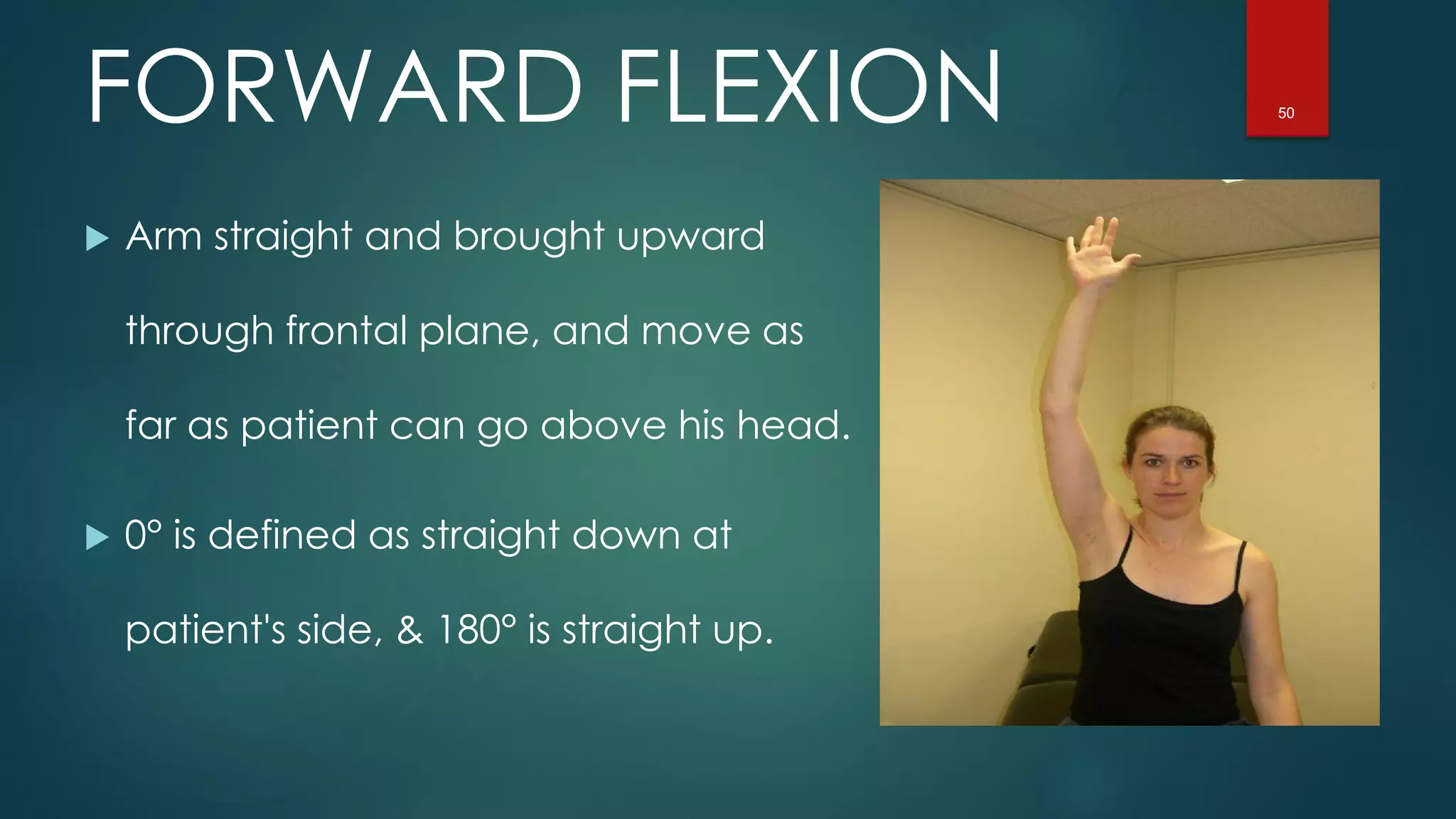
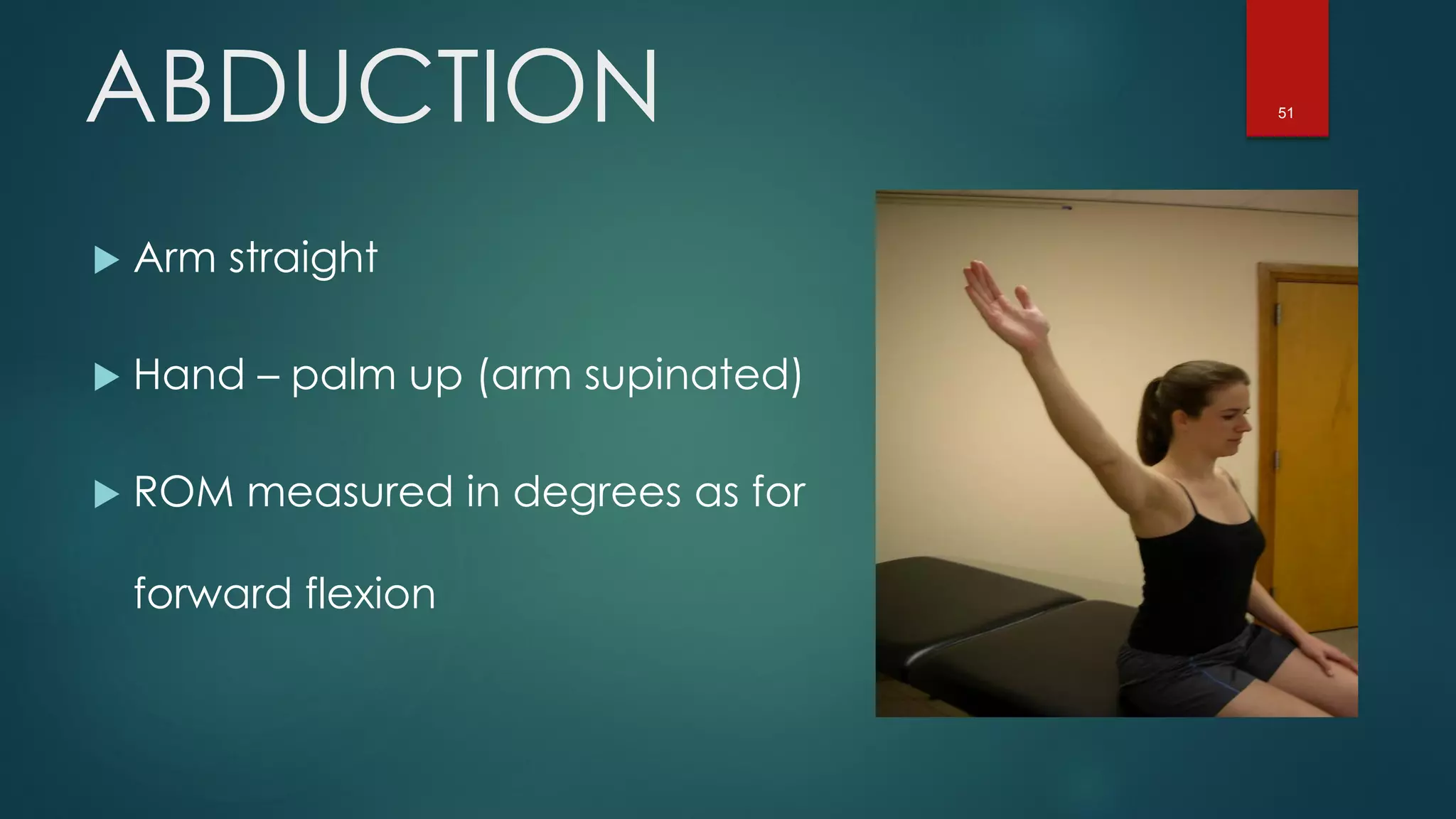
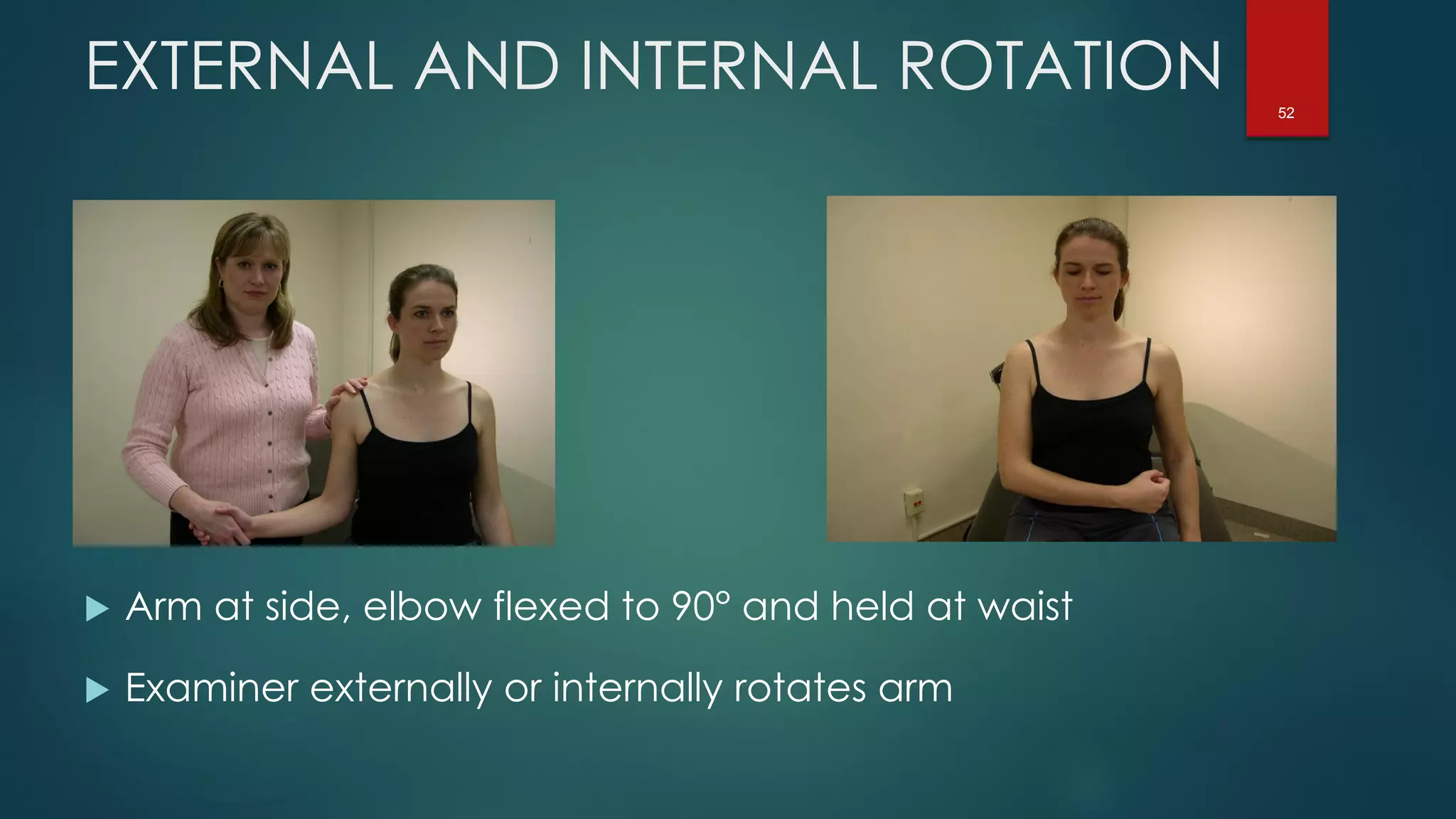
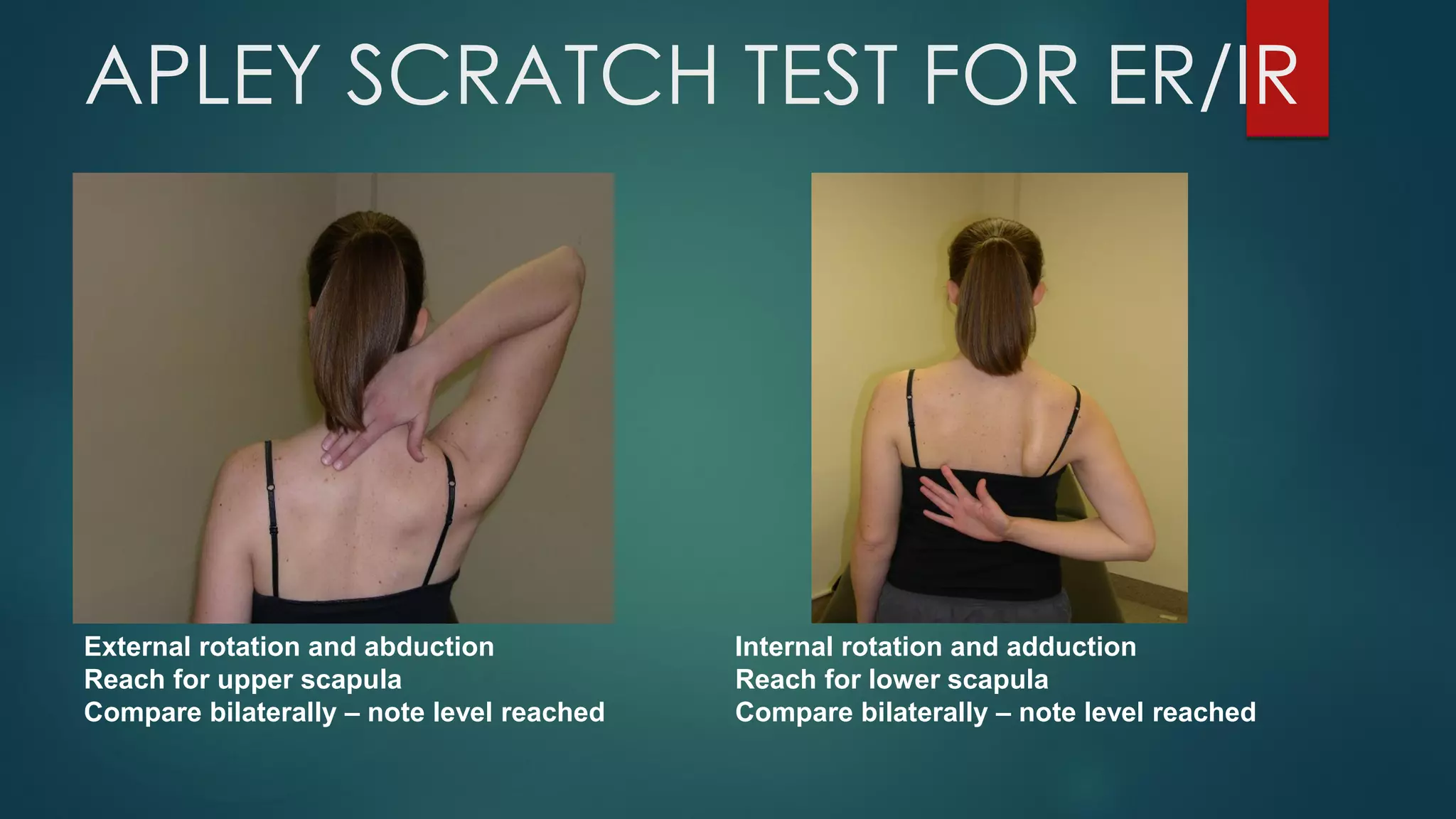
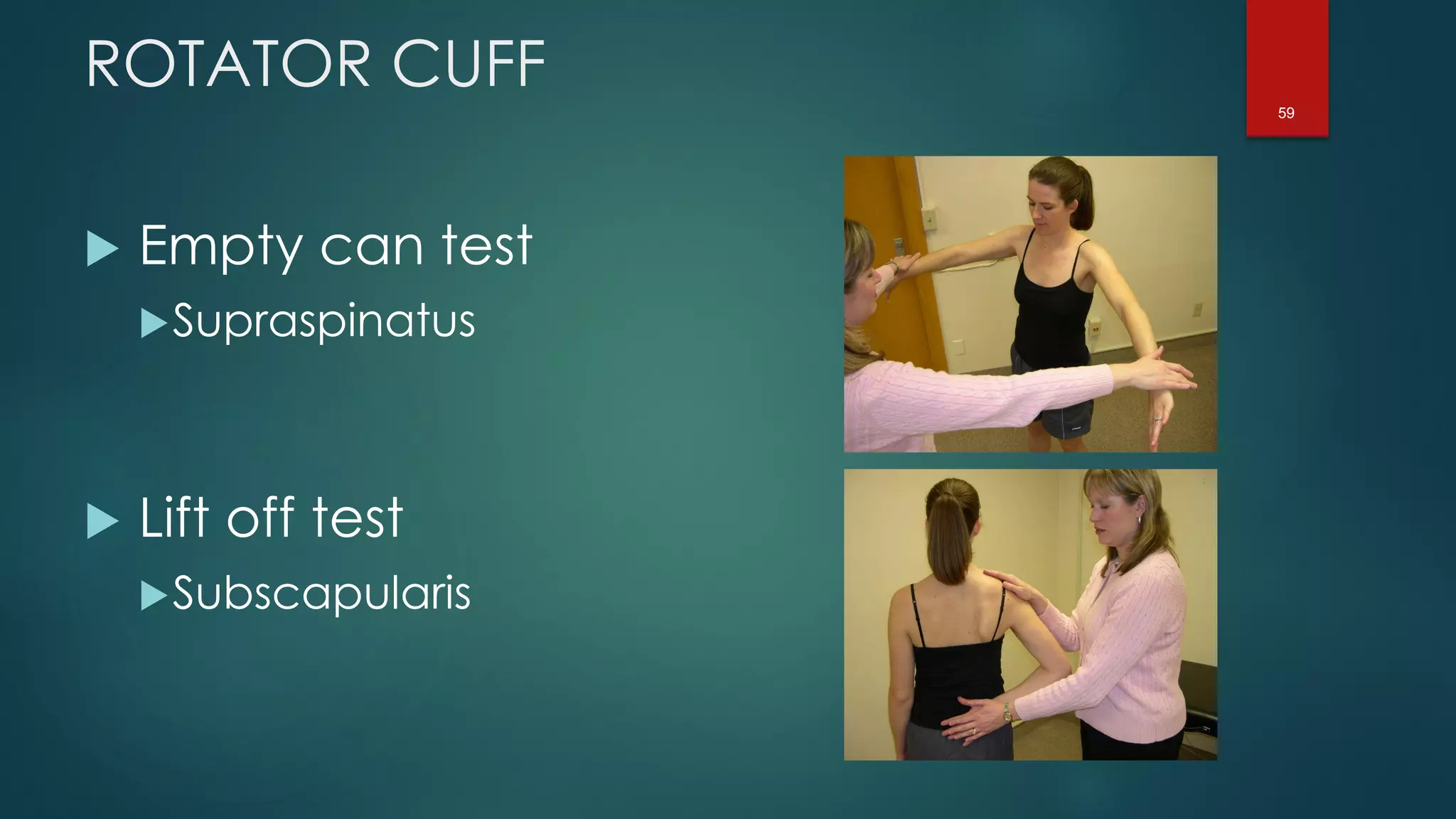
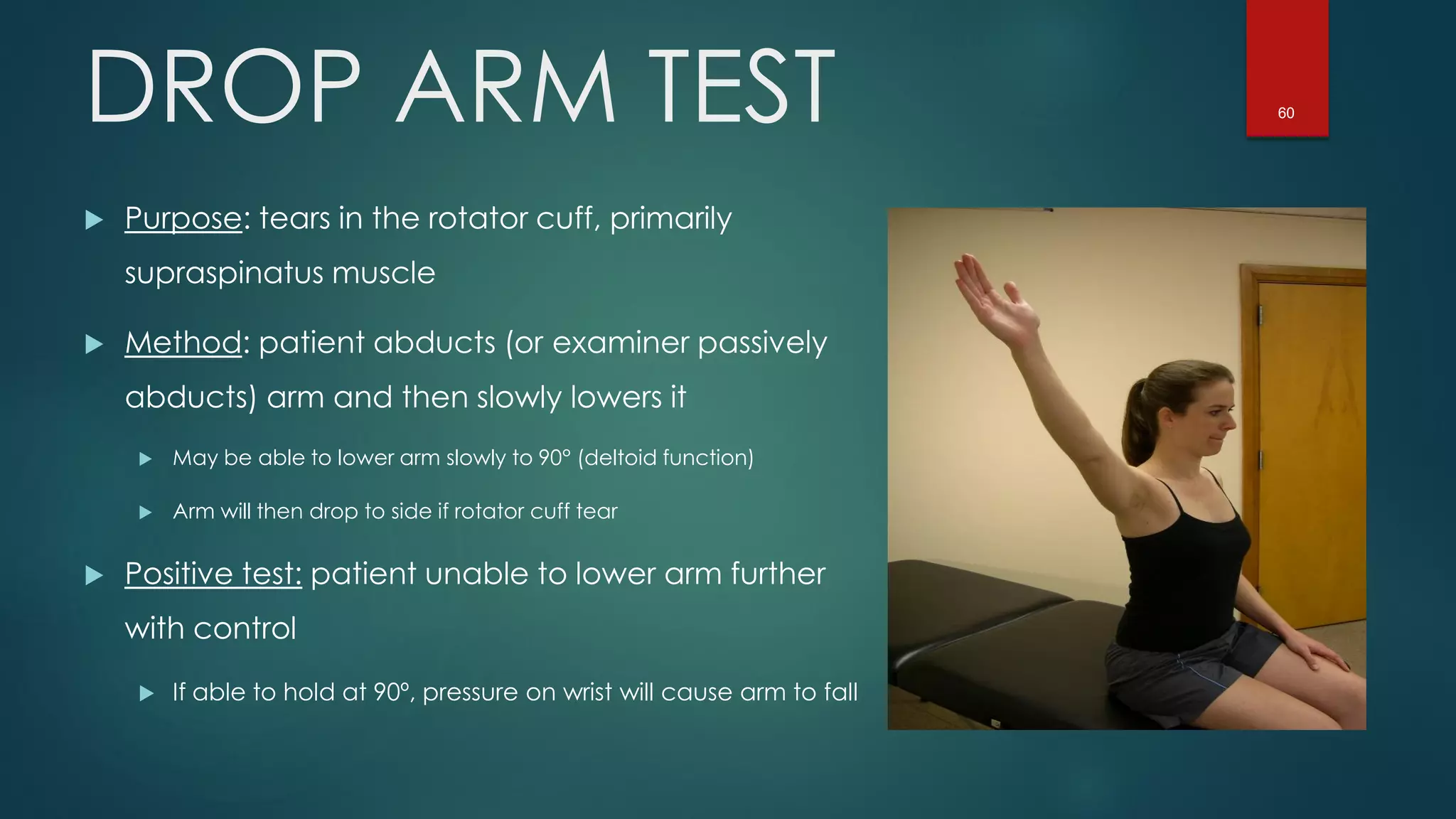
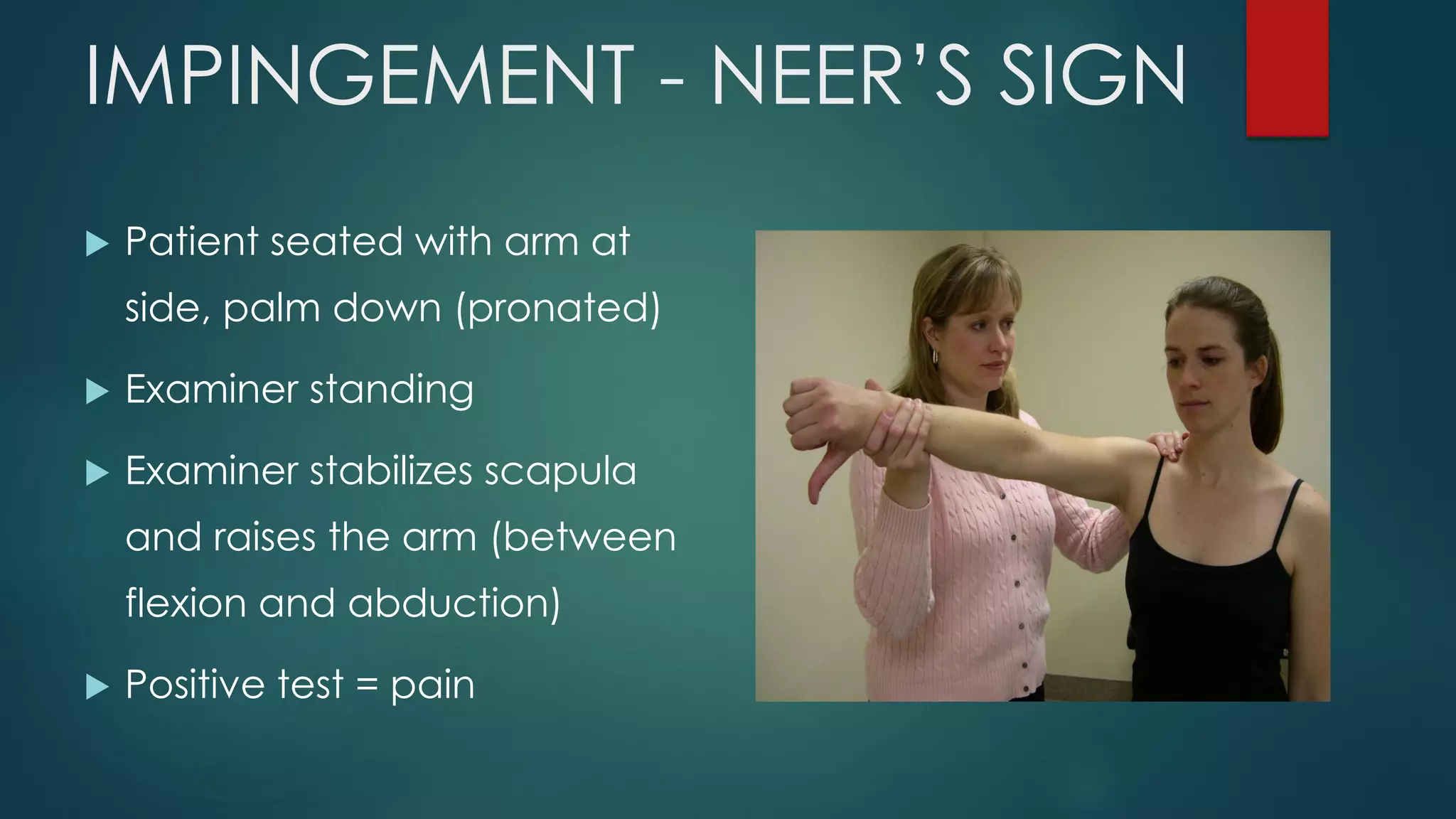
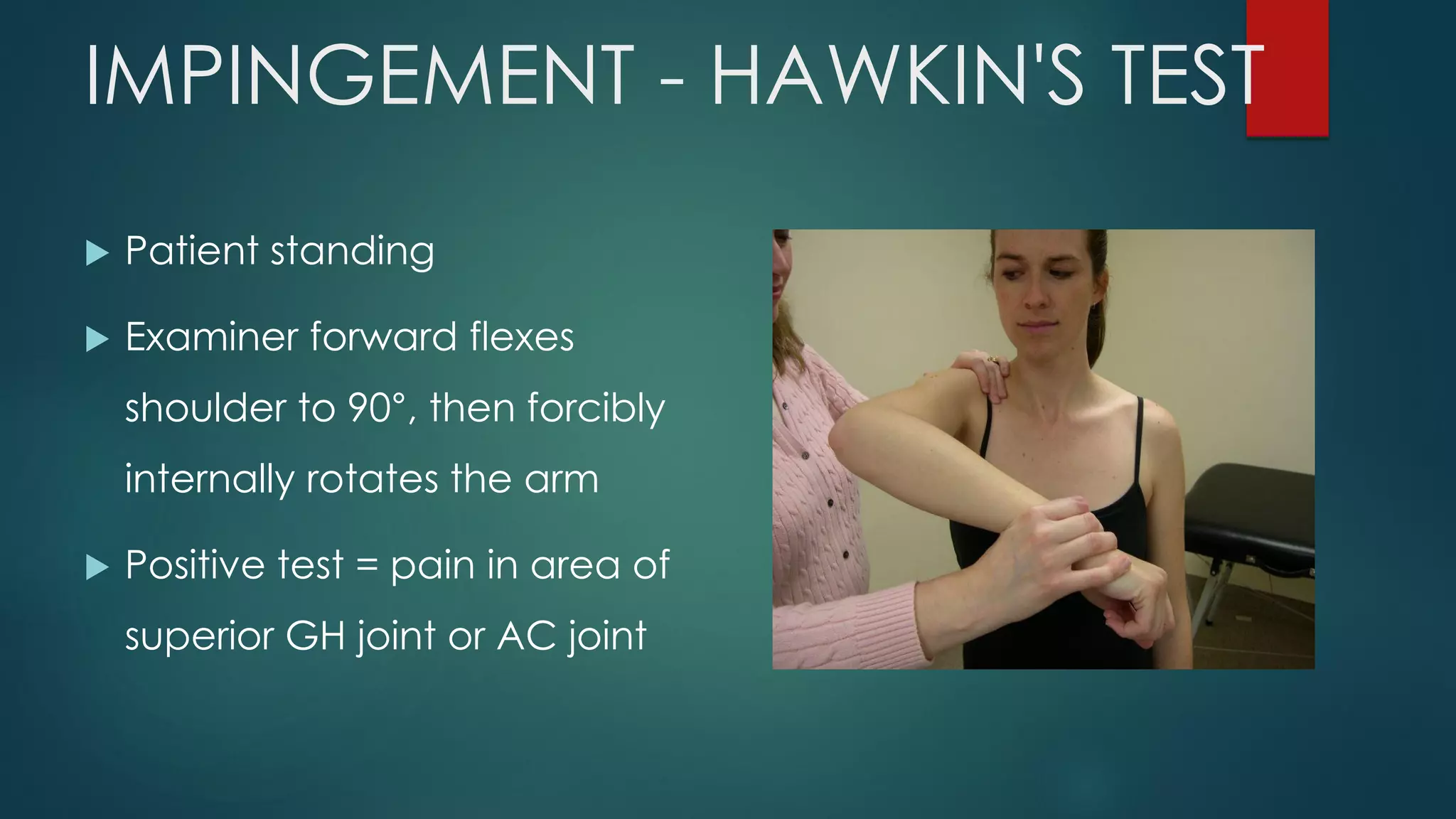
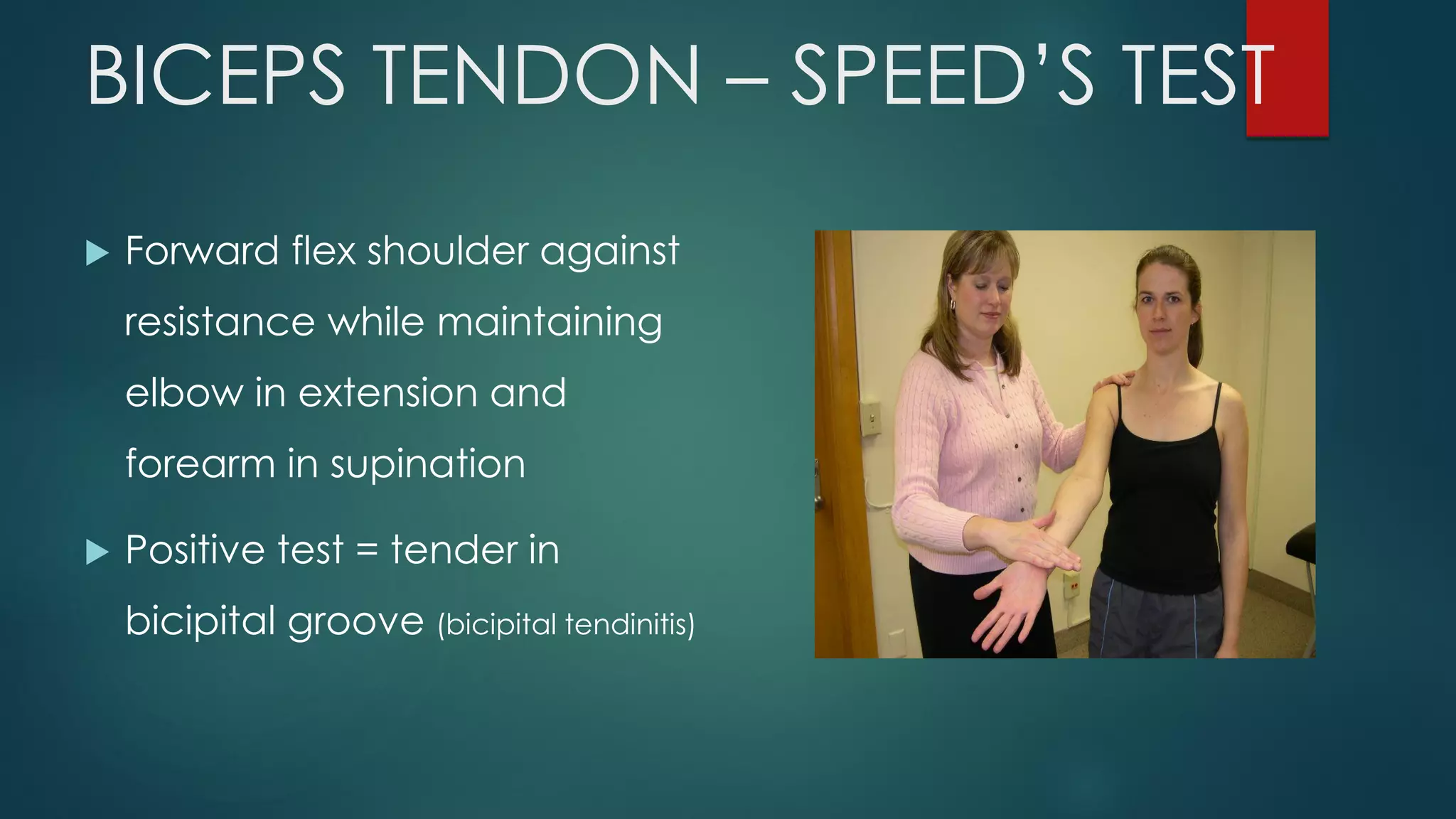
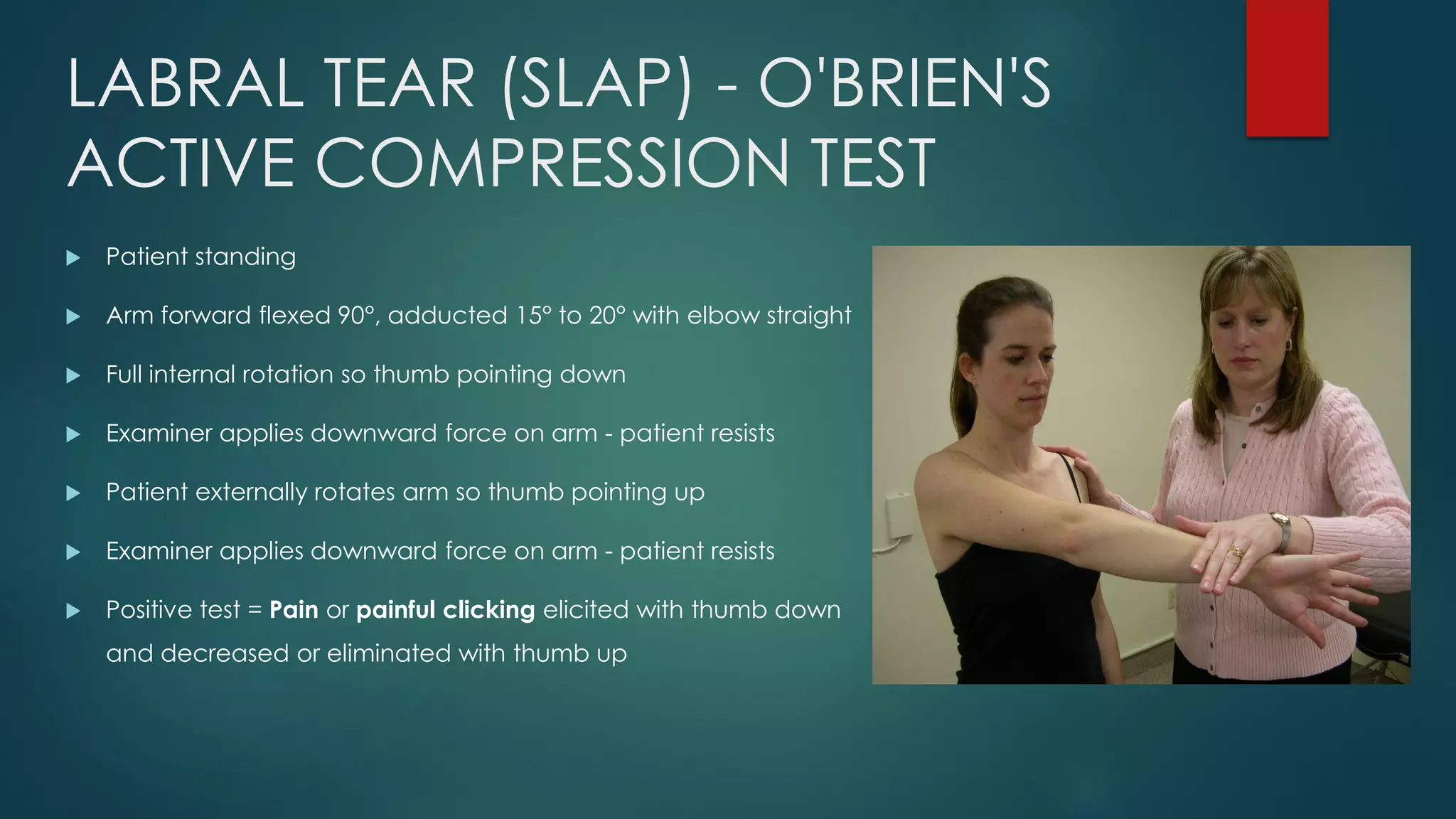
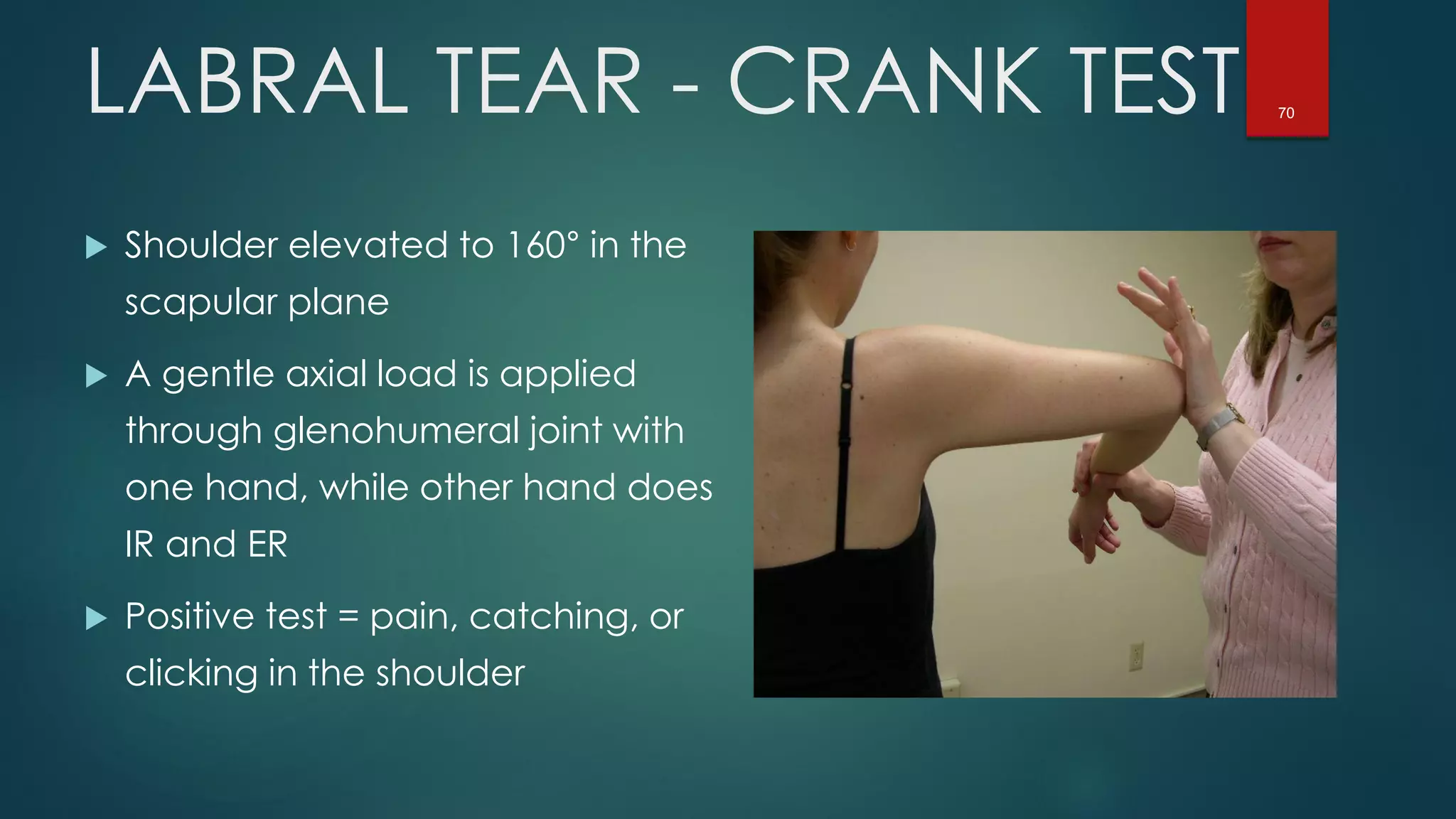
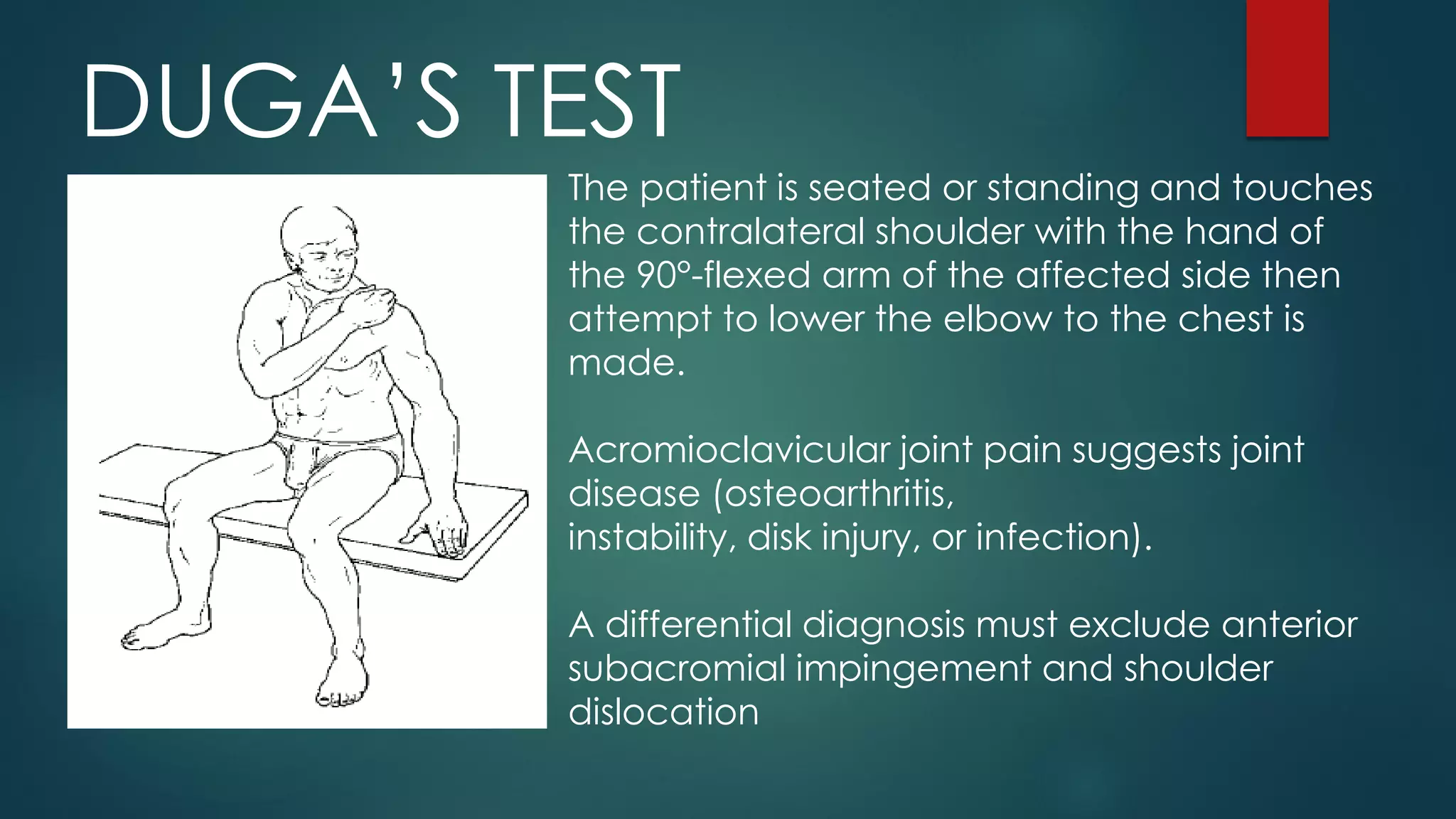
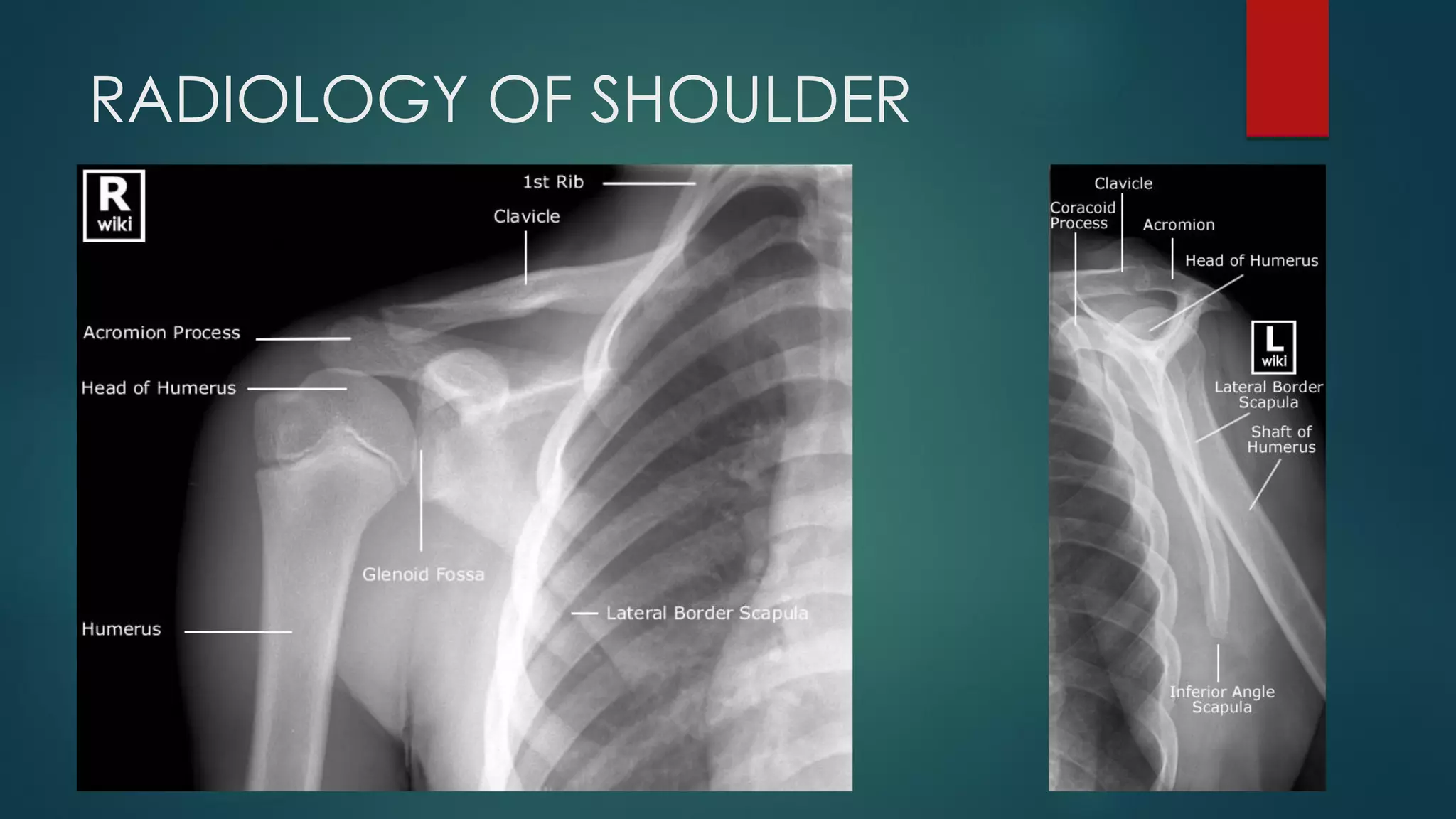
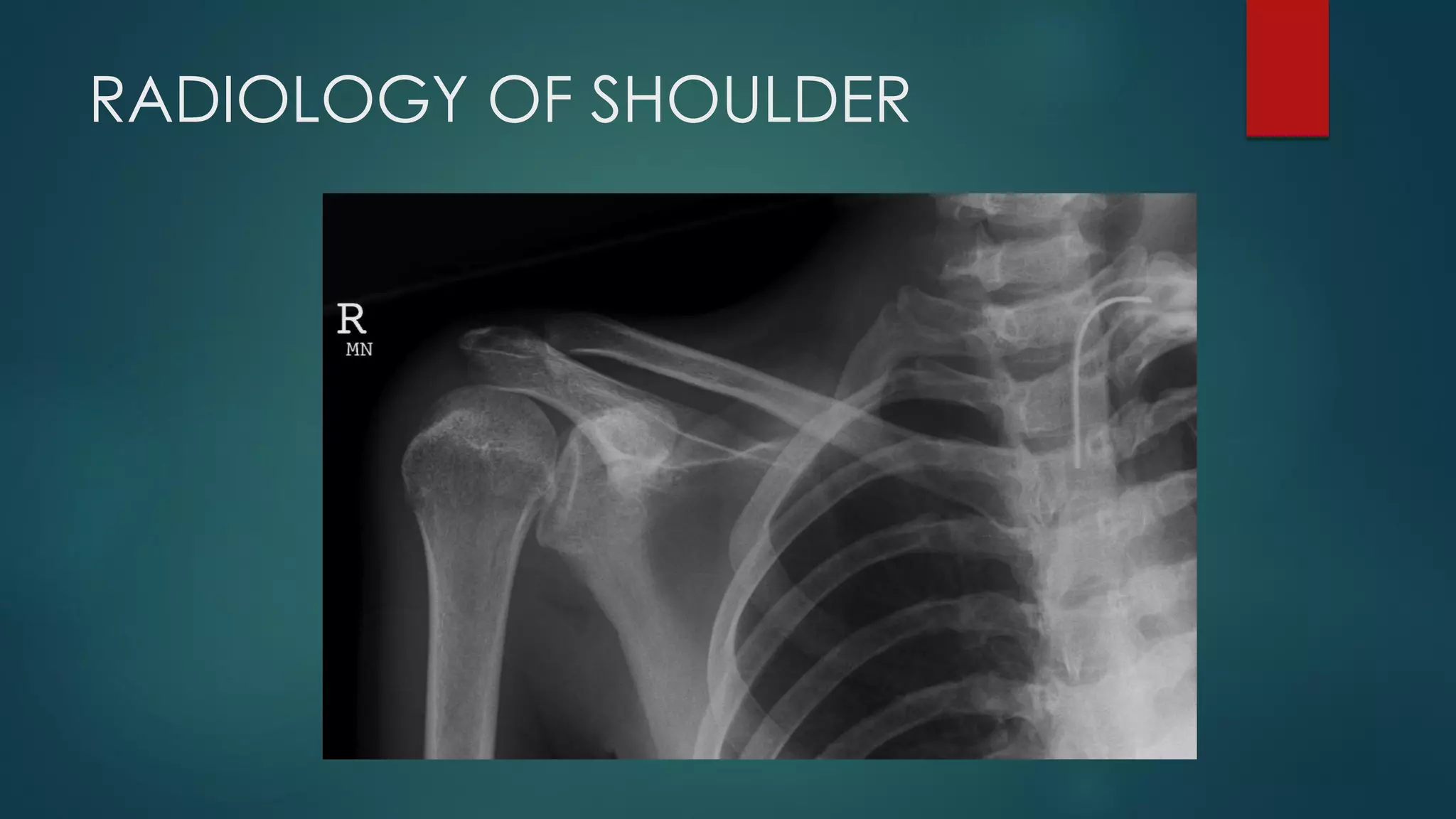
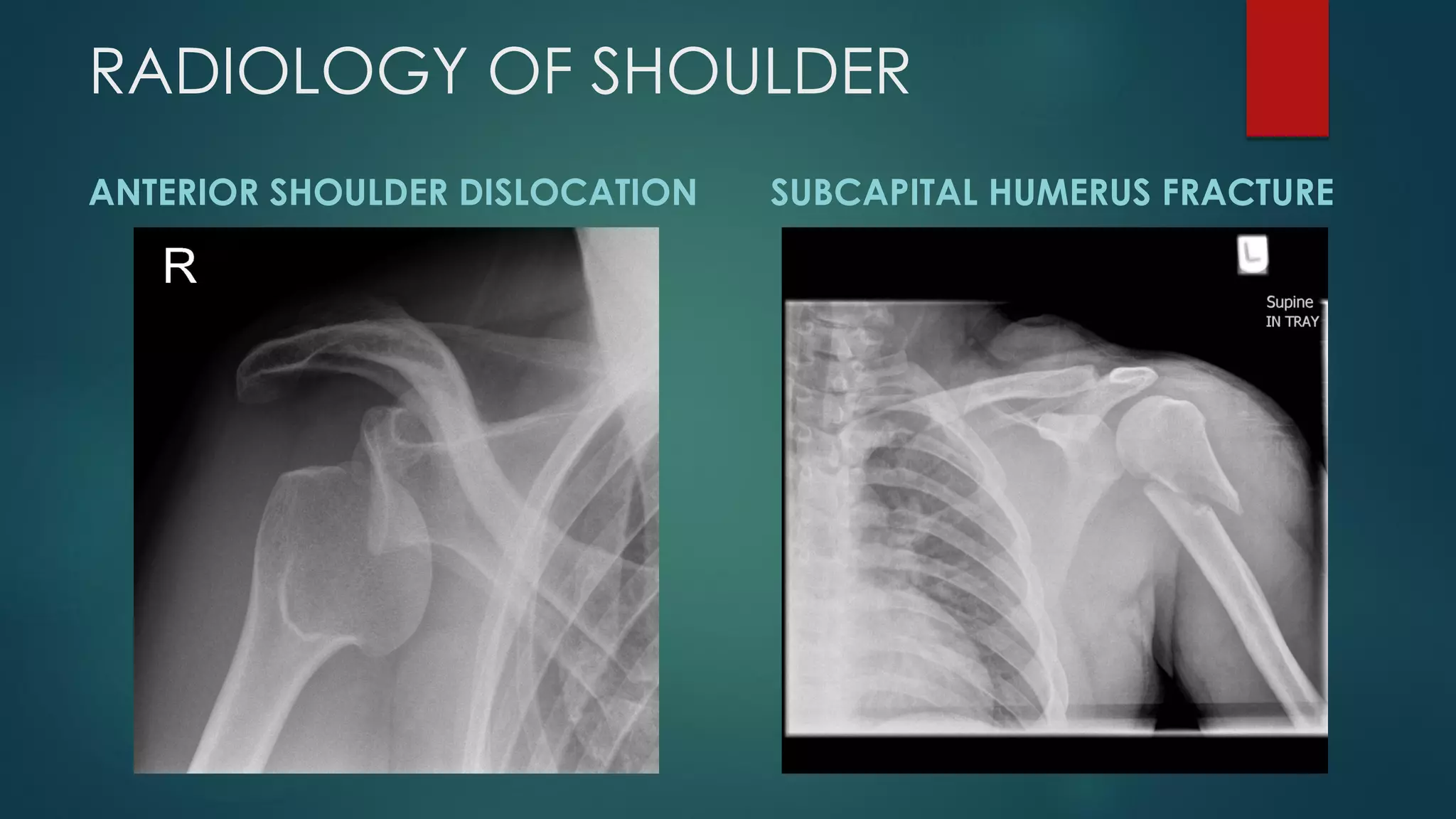
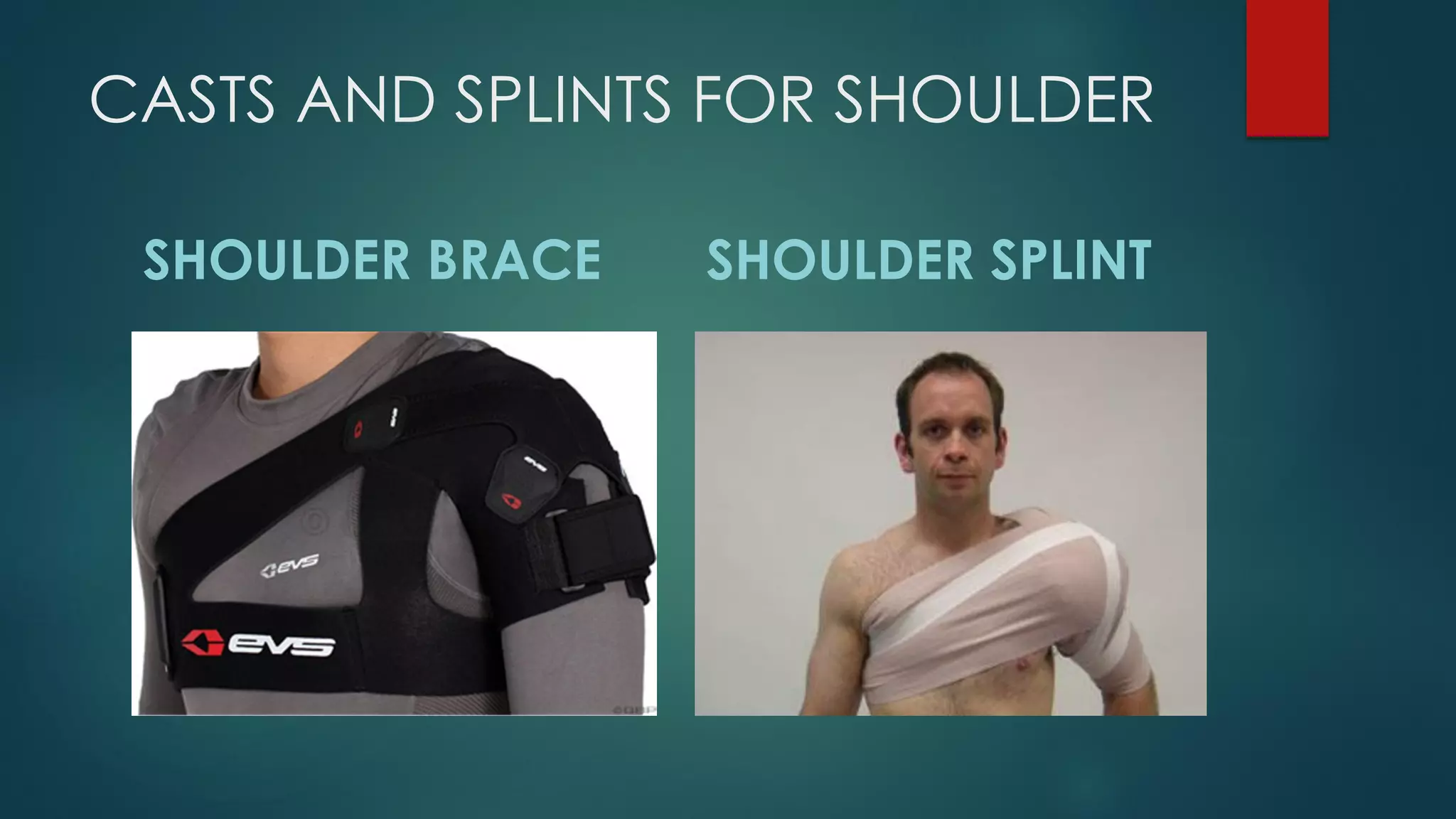


This document provides an overview of performing an exam of the shoulder. It reviews relevant anatomy including bones, joints, ligaments, muscles of the rotator cuff. It describes taking a history including questions about chief complaints, pain characteristics, instability, neurological symptoms, loss of function. The physical exam section reviews inspecting for deformities, palpating various structures, evaluating range of motion including forward flexion, abduction, and rotational movements. Special tests like the painful arc maneuver are also outlined. Differential diagnoses for common shoulder conditions are listed.























































































