Downloaded 205 times
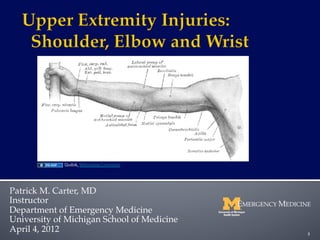








The document reviews key orthopedic injuries of the upper extremities including the shoulder, elbow, and wrist, detailing mechanisms of injury, classifications, diagnosis, and treatment options. It is part of a collaborative effort by the Ghana Emergency Medicine team and is intended for educational purposes, not as a substitute for professional medical advice. Key complications related to these injuries, such as dislocations and fractures, are also discussed.



































































