
Downloaded 83 times

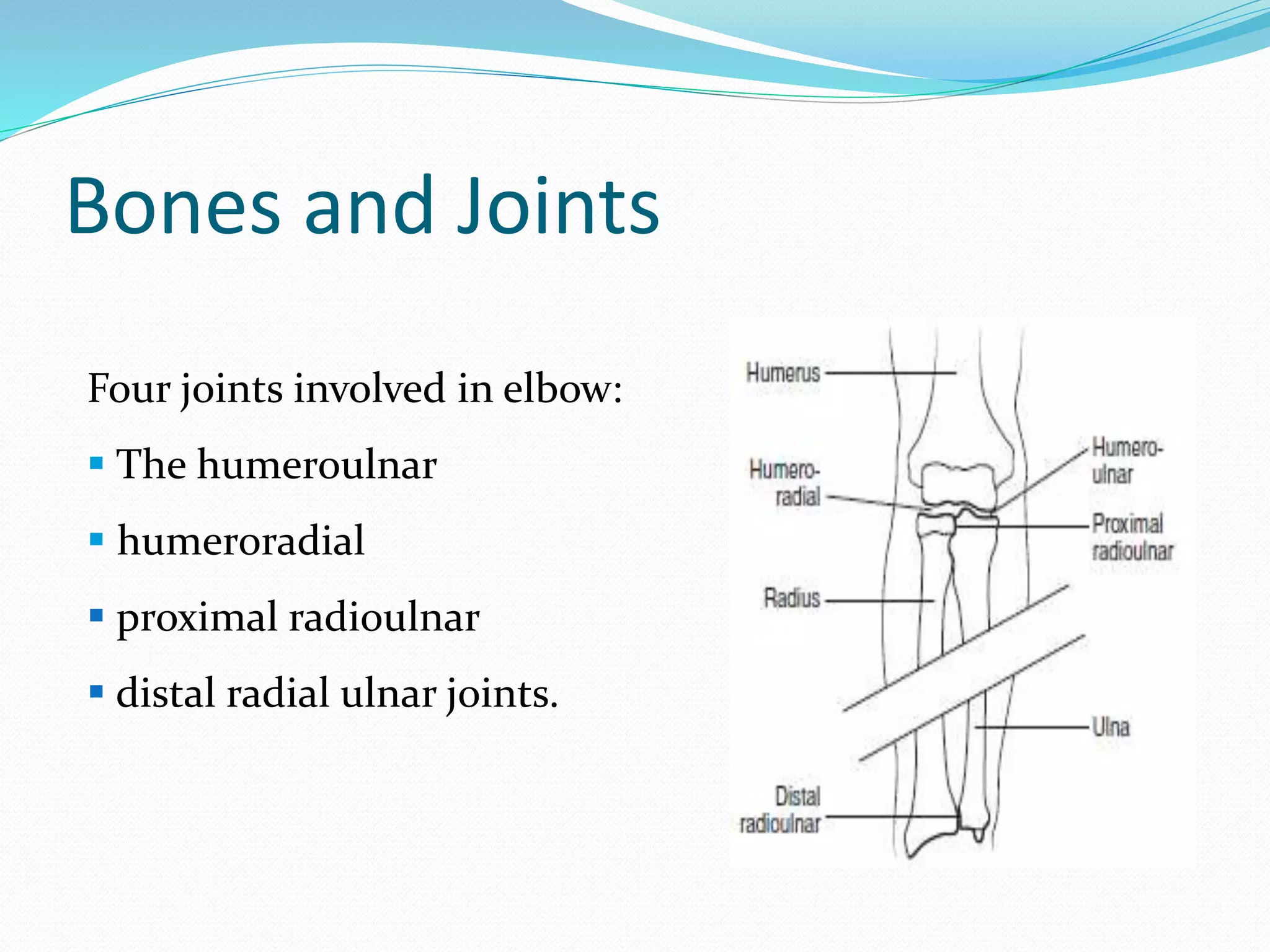






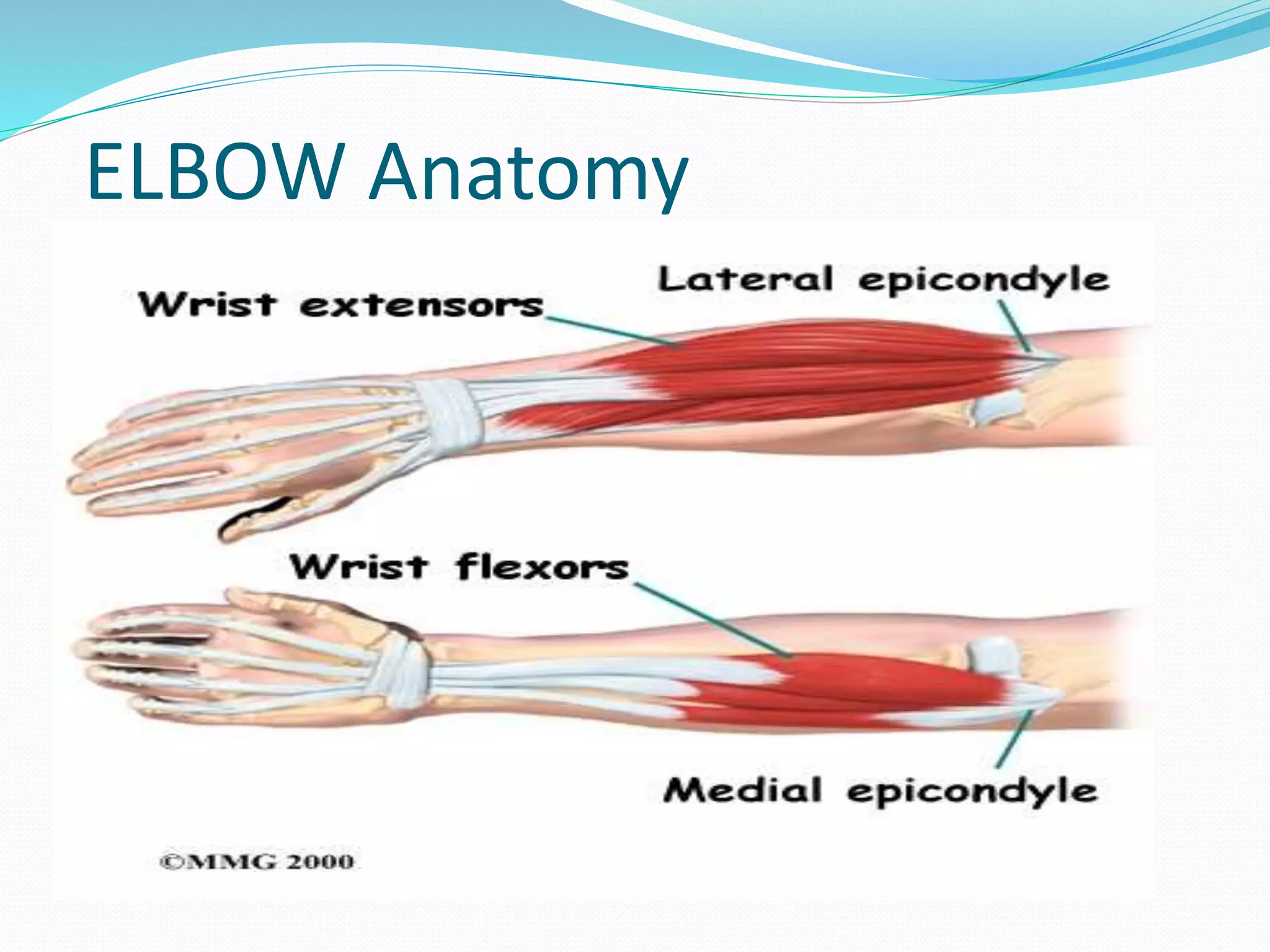


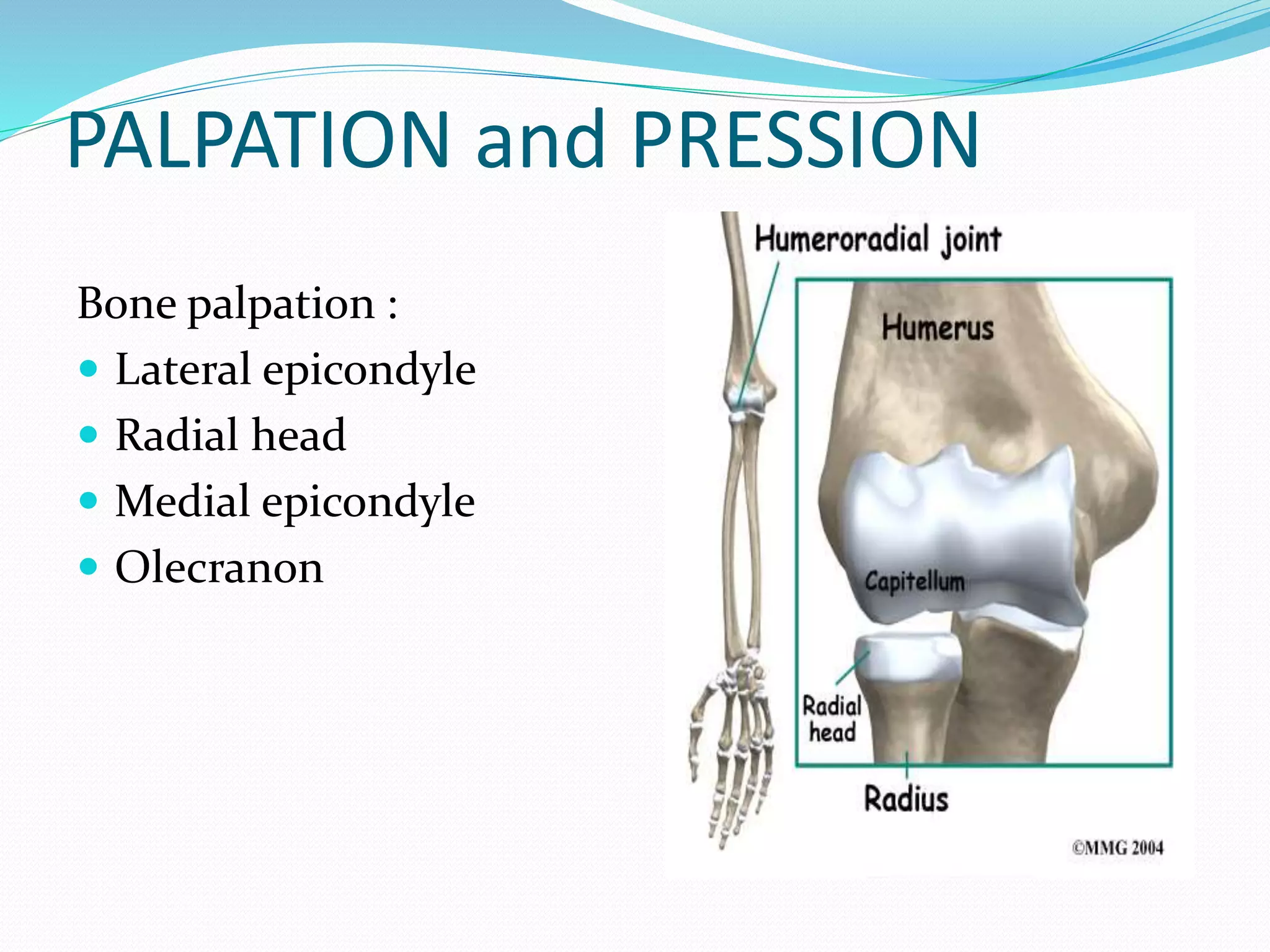
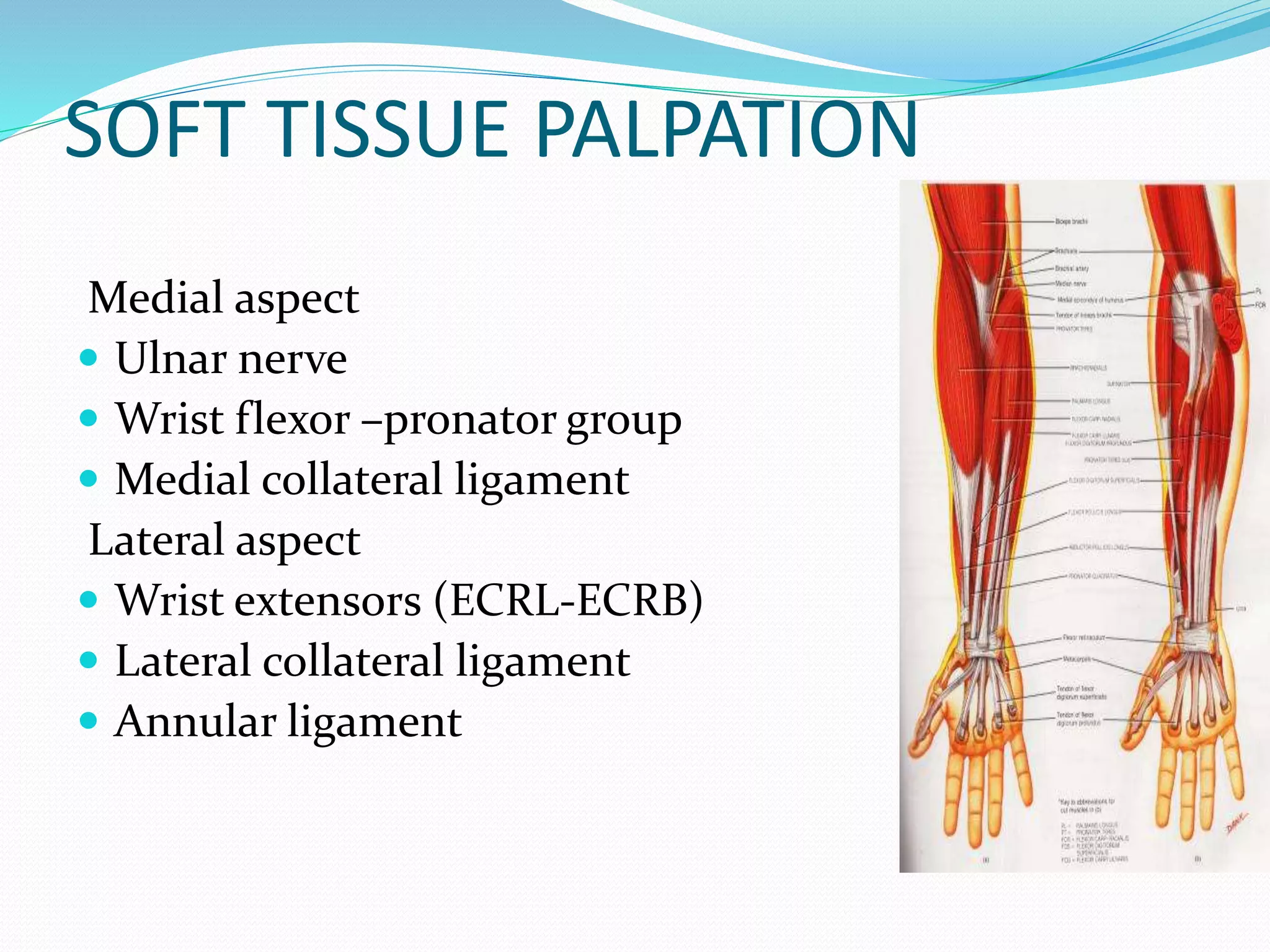


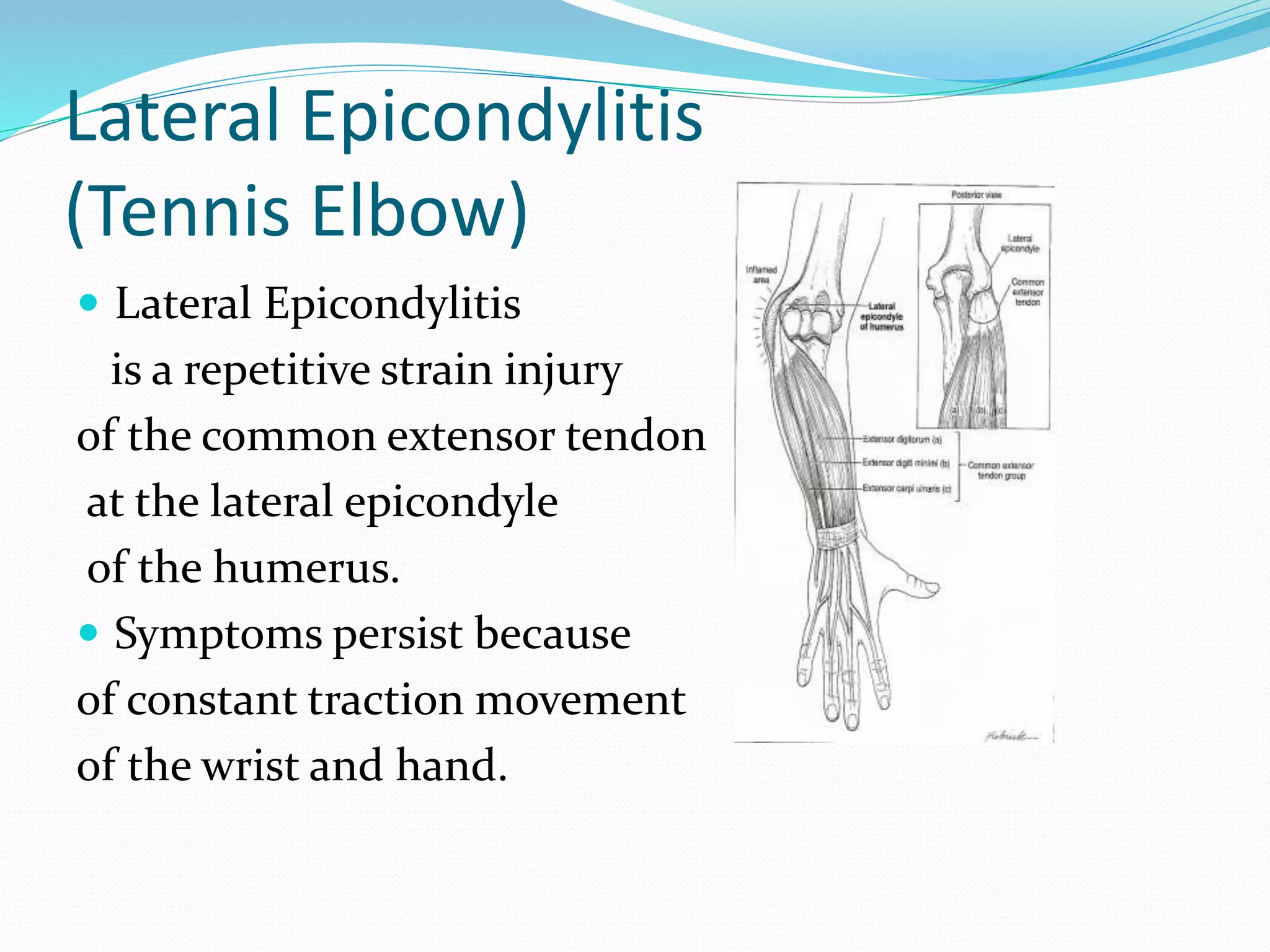
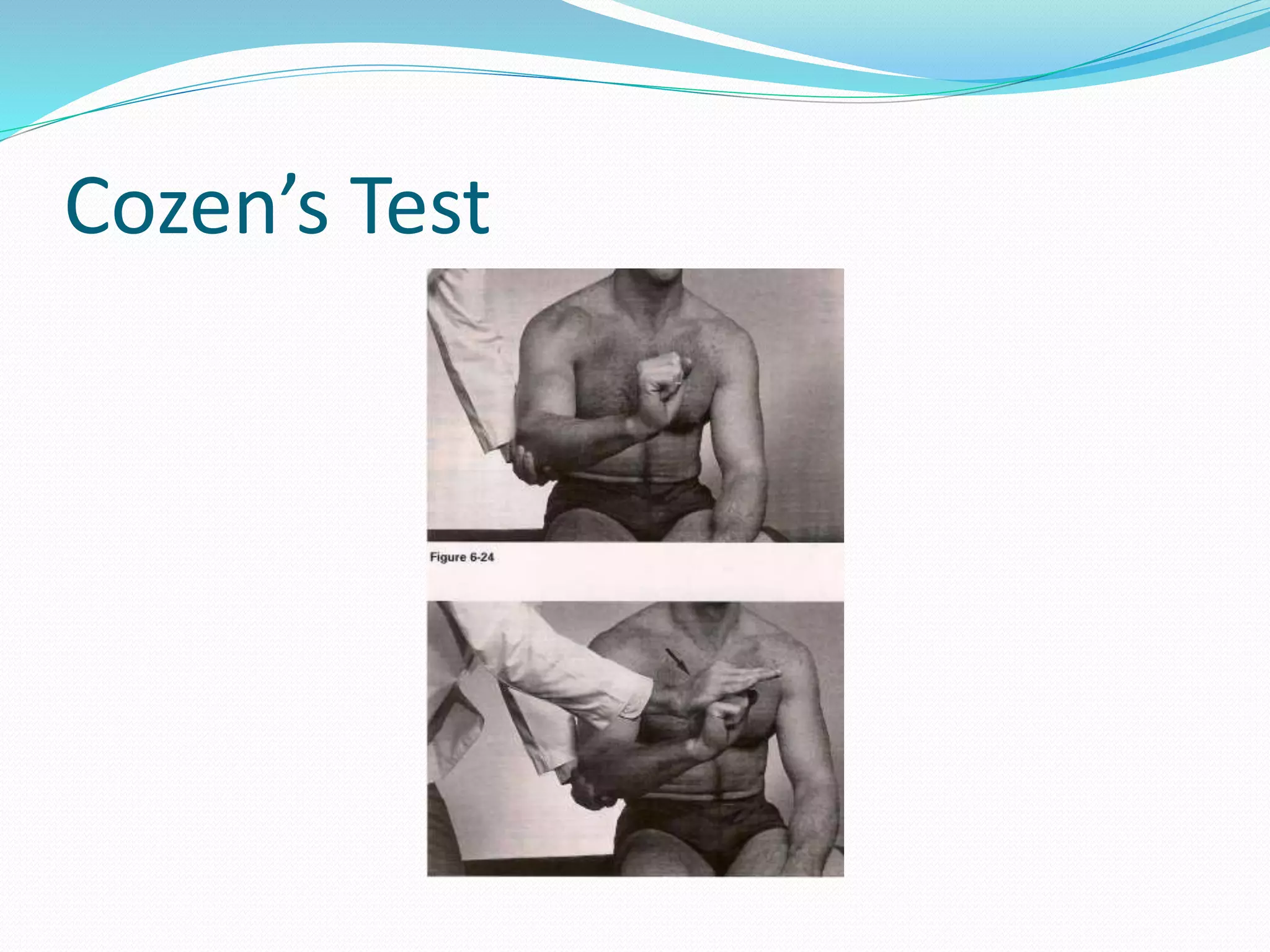

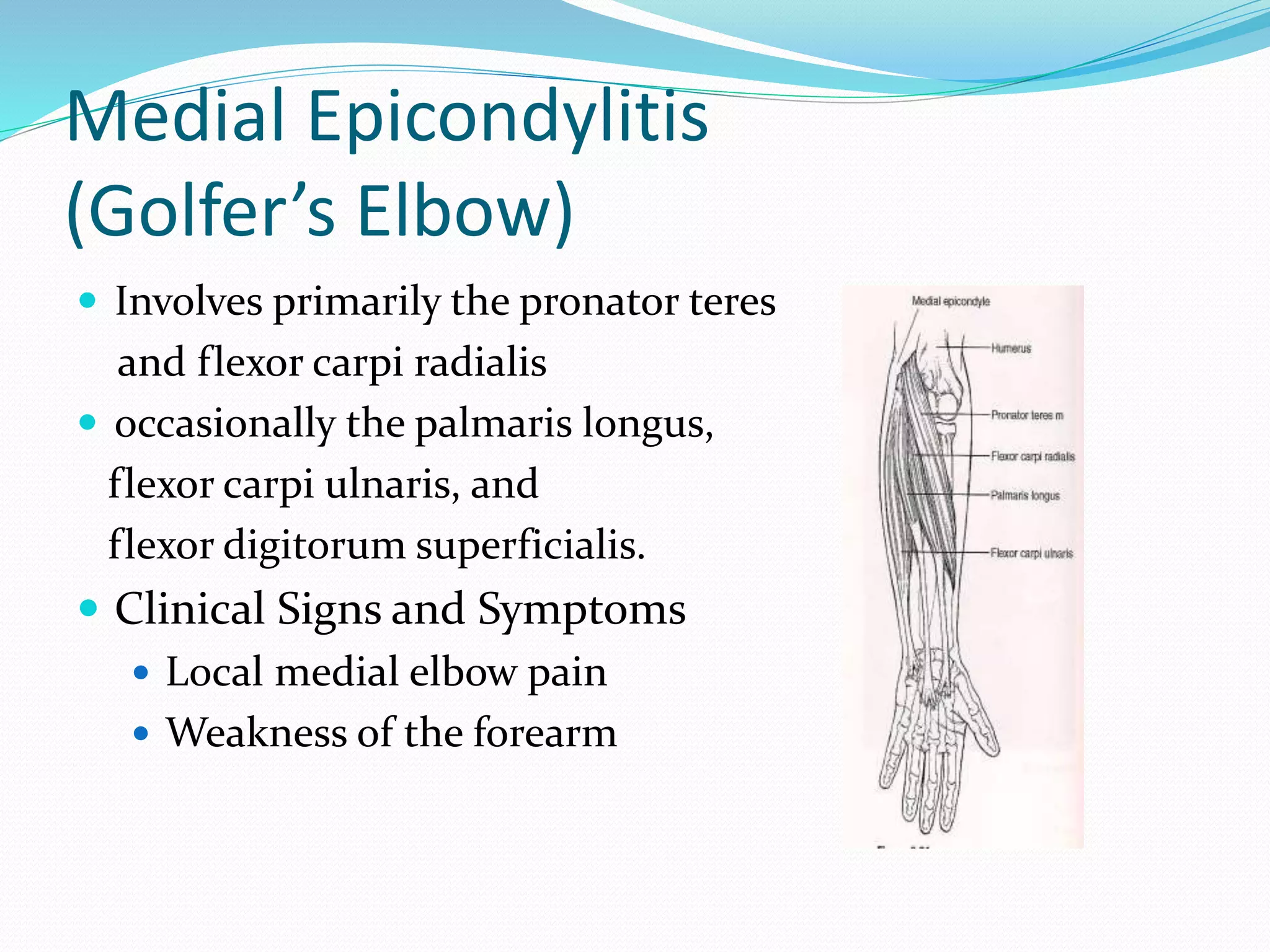
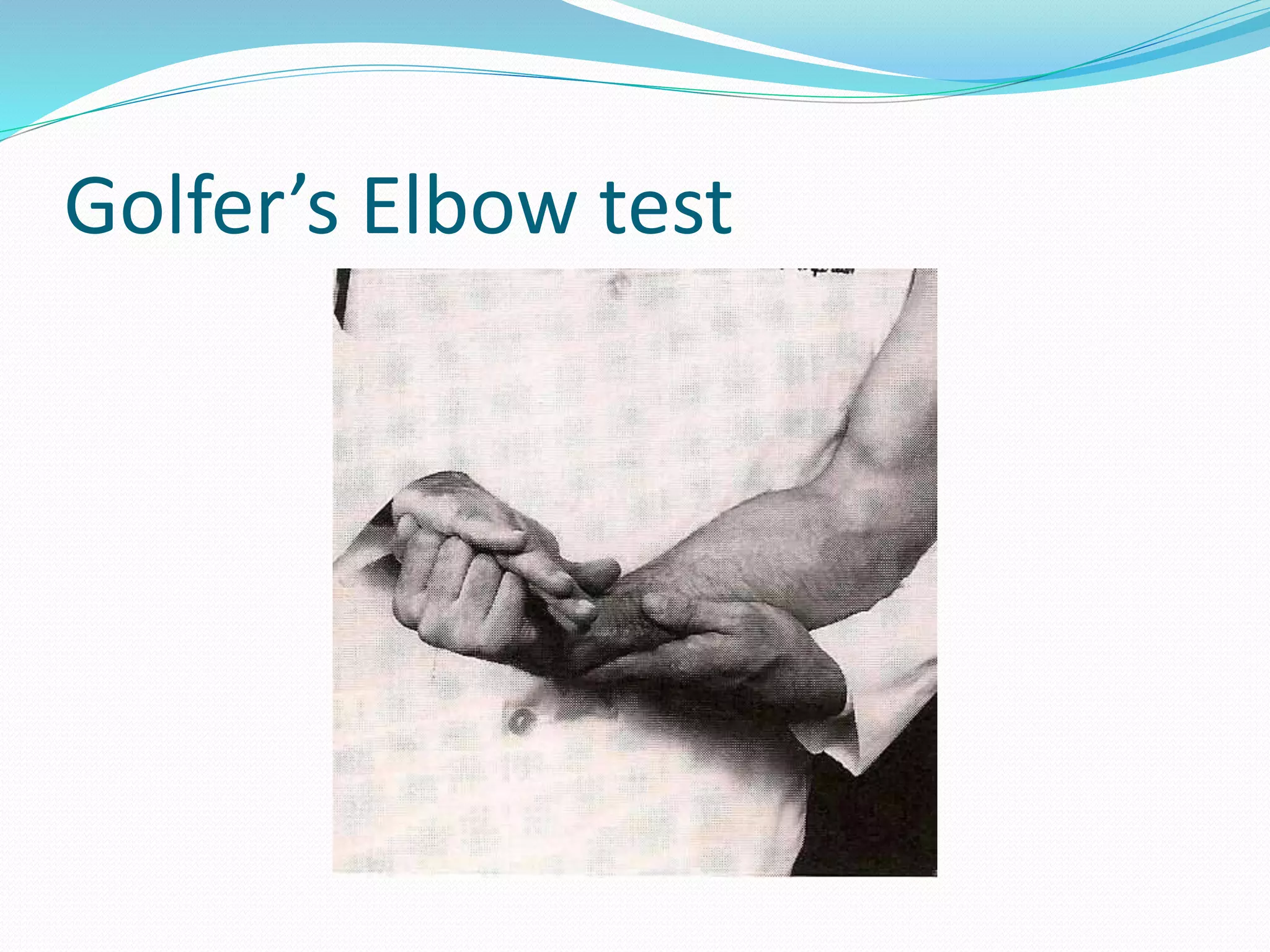








The document provides information on examining the elbow, including: - An overview of elbow anatomy focusing on bones, joints, ligaments and muscles - How to evaluate the elbow through inspection, palpation, range of motion testing and special tests - Common conditions involving the elbow like lateral epicondylitis, medial epicondylitis, ligament instability and neuropathy/compression syndromes - Descriptions of special tests to assess for these conditions like Cozen's test, Golfer's elbow test, varus/valgus stress tests and Tinel's sign























































































