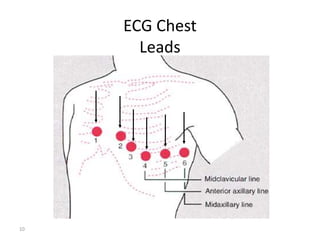
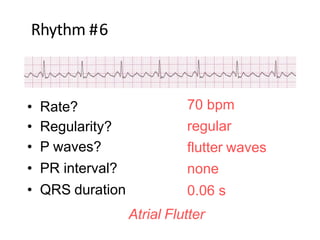
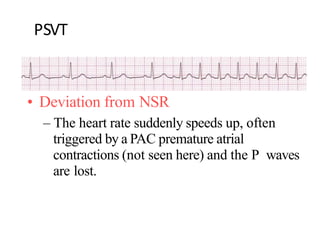
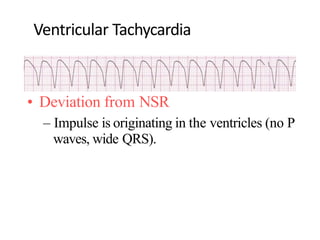
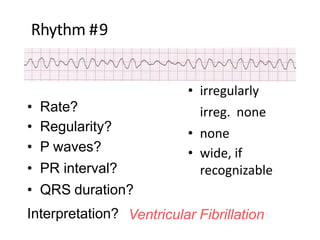
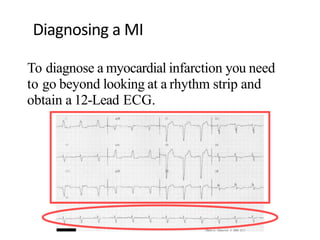
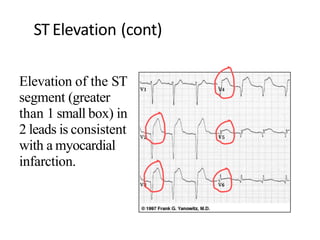
The document discusses the basics of electrocardiography (ECG), including the 12-lead ECG system and cardiac rhythms. It explains that a standard ECG uses 6 limb leads (I, II, III, aVR, aVL, aVF) and 6 precordial/chest leads (V1-V6). It describes Einthoven's triangle and law. It discusses normal sinus rhythm, cardiac intervals, axis determination, hypertrophy, ischemia, blocks, arrhythmias, and bundle branch blocks. Key points are made about rate, regularity, P waves, PR interval, and QRS duration for interpreting rhythms.