Downloaded 19 times
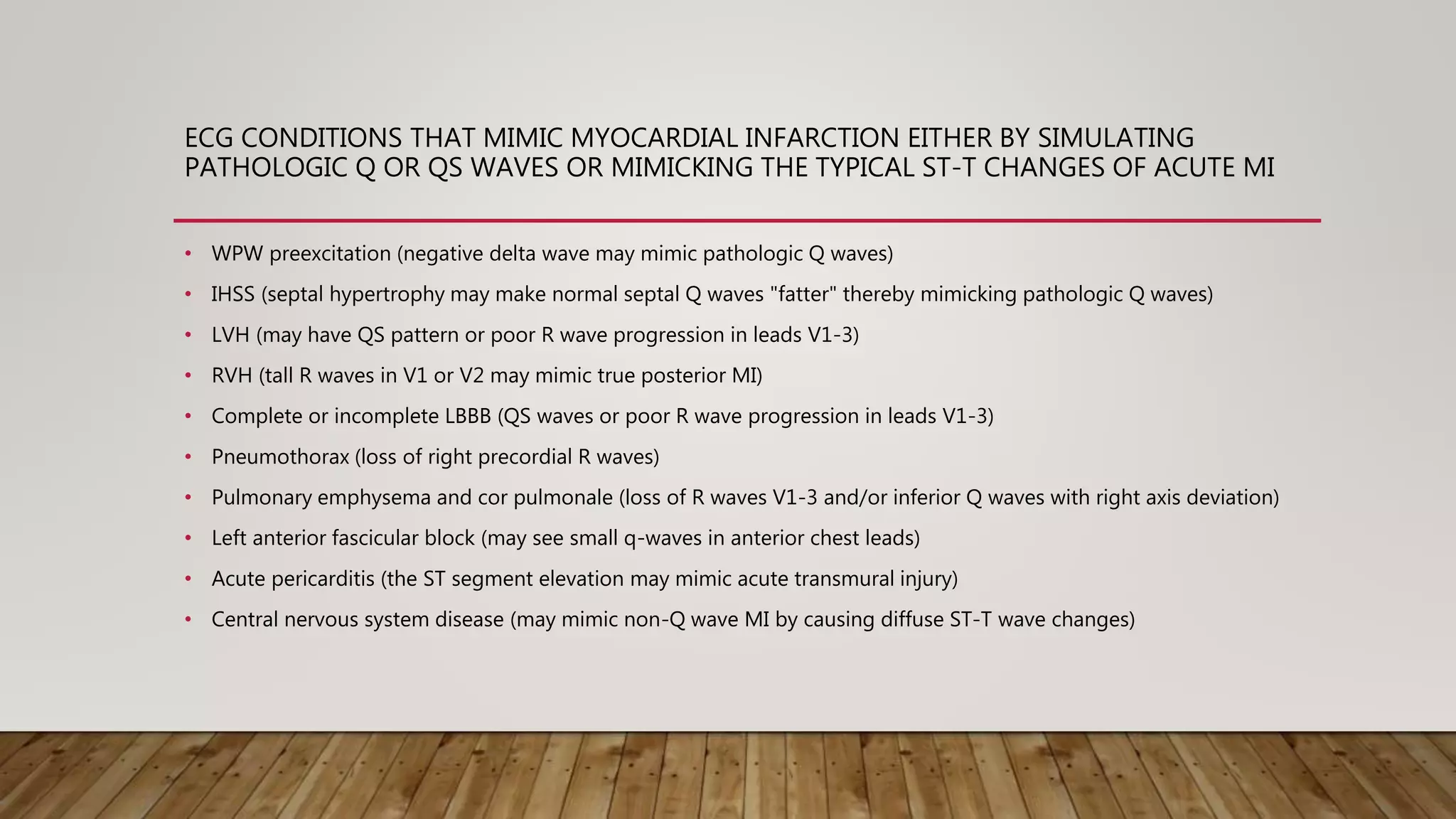
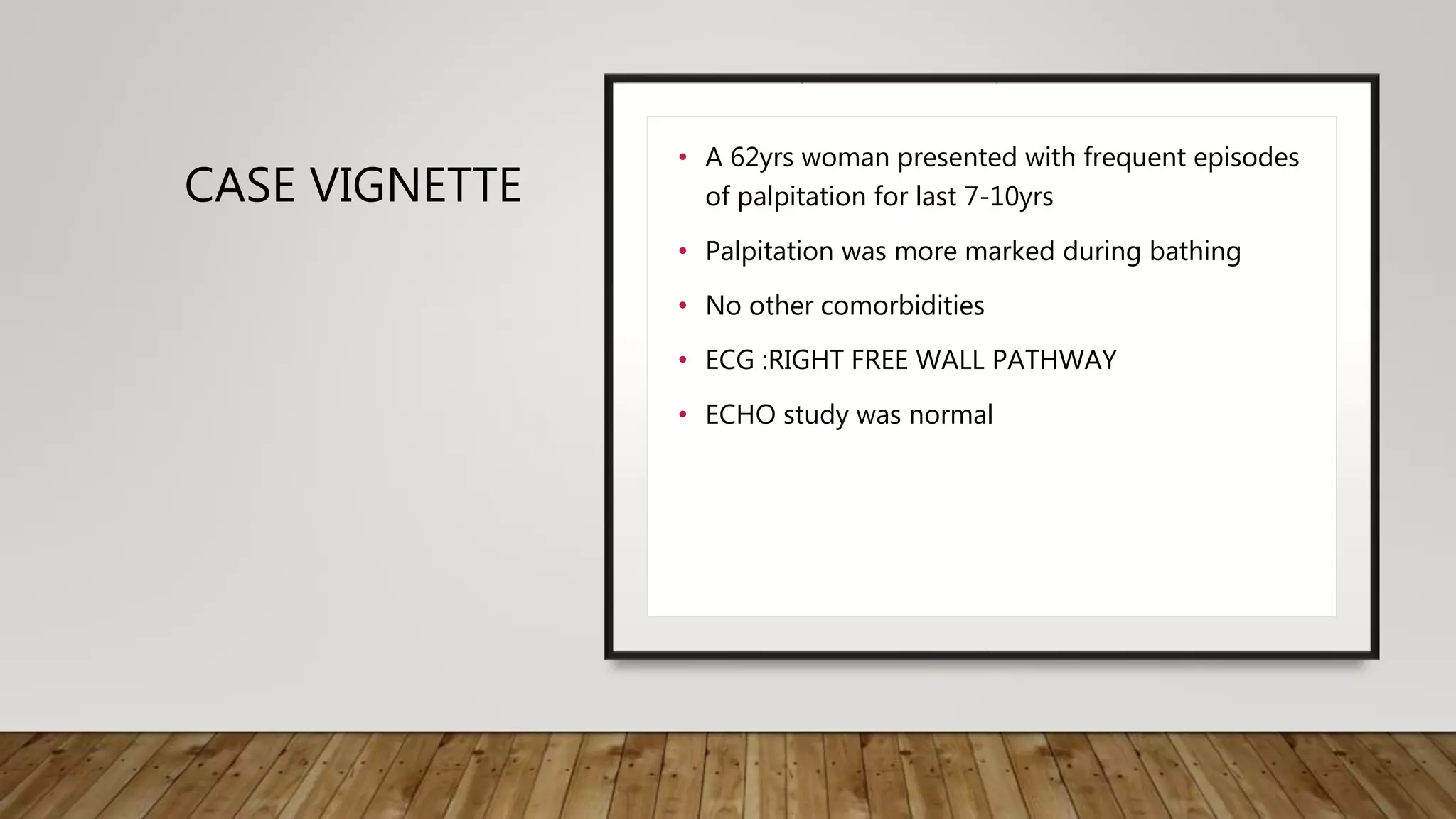



The document discusses conditions that can mimic myocardial infarction through changes in ECG readings, including WPW preexcitation, IHSS, LVH, and others. A case vignette illustrates a 62-year-old woman with a unique ECG pattern indicative of Wolff-Parkinson-White syndrome. The document emphasizes the importance of accurate ECG interpretation to differentiate these conditions.












































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)










