Downloaded 39 times
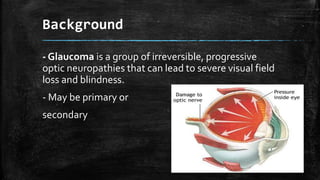

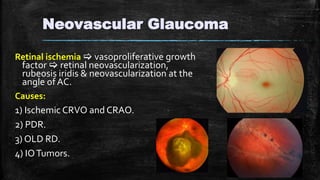
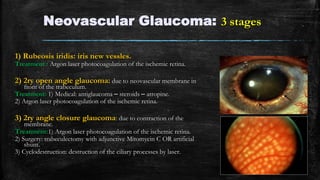
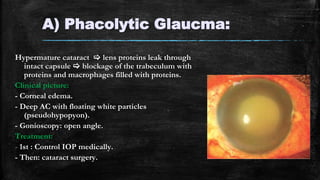



The document discusses secondary glaucoma, a condition where known ocular or non-ocular disorders affect aqueous outflow, leading to increased intraocular pressure (IOP). It outlines various classifications, including angle closure and open-angle types, along with key conditions such as pseudoexfoliation glaucoma and neovascular glaucoma. Treatment strategies are also summarized, depending on the specific type of secondary glaucoma identified.























































































