Download to read offline


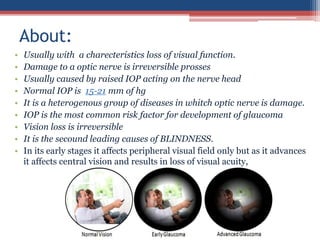
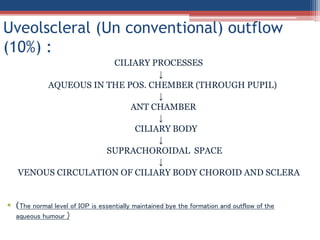
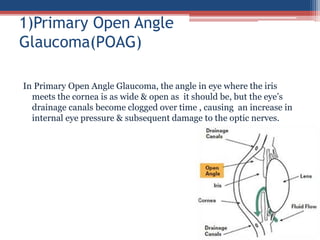
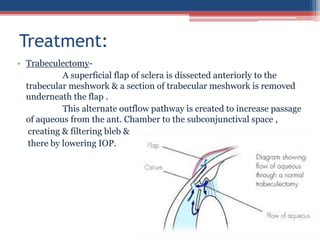
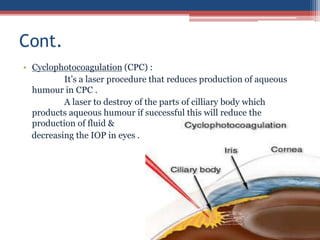


The document discusses glaucoma, a progressive optic nerve disease characterized by elevated intraocular pressure (IOP) and irreversible vision loss if untreated. It covers its classification, causes (primary, secondary, congenital), risk factors, symptoms, clinical features, investigative methods, and treatment options including surgical and laser interventions. Significant attention is given to the pathophysiology, progression, and management of various types of glaucoma.

































































