Download to read offline
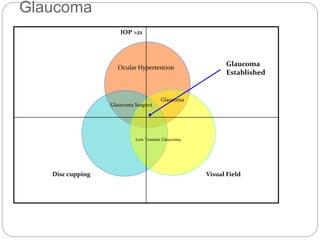
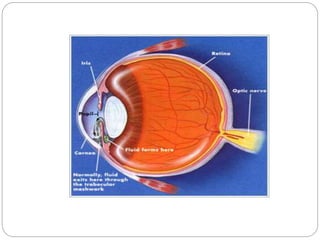
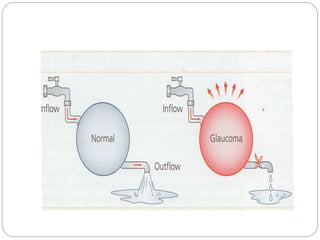
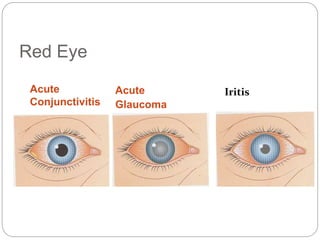
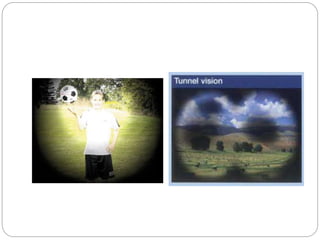
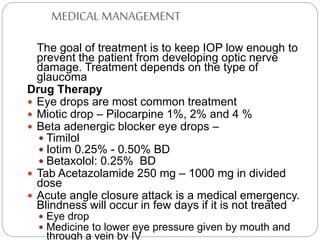
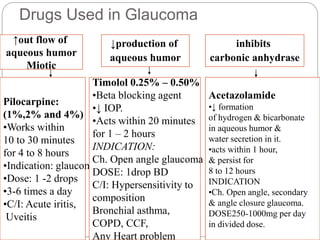


Glaucoma is a group of eye diseases characterized by increased pressure in the eye due to excess fluid. If left untreated, it can cause damage to the optic nerve and result in vision loss and blindness. The two most common types are open-angle glaucoma, which develops slowly over time, and angle-closure glaucoma, which develops acutely and requires urgent treatment to prevent vision loss. Treatment involves medications or surgery to lower eye pressure and prevent further damage to the optic nerve. Nursing care focuses on administering eye drop medications correctly, providing a safe environment, teaching patients self-care techniques, and ensuring follow-up medical care.


































































