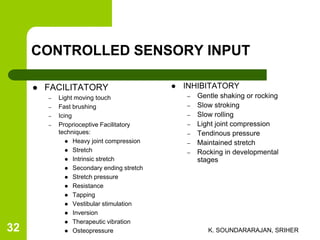
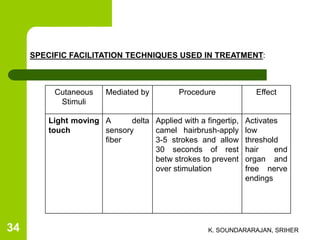
The document discusses Margaret Rood's approach to neurorehabilitation, which uses controlled sensory input to facilitate motor control. Rood believed motor functions develop from primitive reflexes through stimulation of appropriate sensory receptors. Her approach uses techniques like light touch, brushing, icing, stretching, resistance, tapping, and vestibular stimulation to activate cutaneous and proprioceptive receptors. While Rood's theory aimed to improve motor function, some aspects are outdated and more research is needed to evaluate the physiological effects of her techniques.