Download as PPSX, PPTX


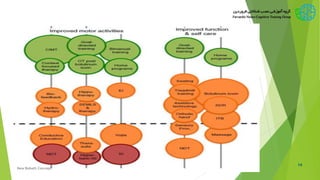

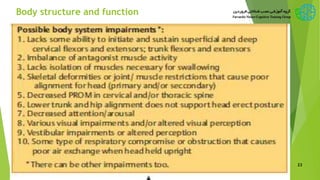

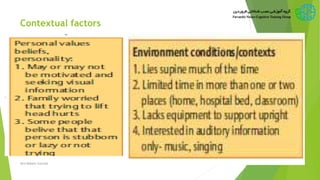
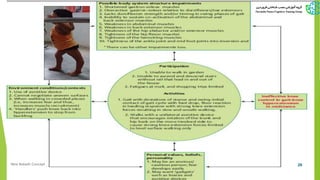
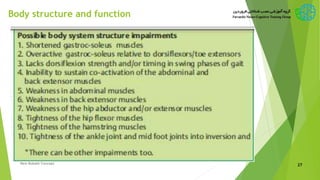



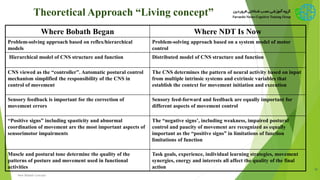


The New Bobath Concept (NDT) focuses on the advanced examination and treatment of individuals with movement and postural control disturbances due to central nervous system lesions, primarily in children with cerebral palsy. It emphasizes a holistic, interdisciplinary approach informed by current research, aiming to enhance individual participation and activity by addressing impairments through therapeutic handling and individualized interventions. Critics point out challenges in demonstrating superiority over alternative treatments and inconsistency in outcomes related to the therapy's effectiveness across various domains.























































































